Annals ofthe MBC - vol. 2 - n' 3 -
September 1989
THE LOW AIR LOSS
BED SYSTEM IN TREATMENT OF BURN PATIENTS
Landi, 0., Catrani S., Mengozzi E, Greco 1, Erbazzi A.,
Arcangeli F., Feletti S.
Civisione Dermatologica, Centro Ustioni, Ospedale
Bufalini, USL 39, Cesena, Italia
SUMMARY.
In the new Mediscus Mark 5A-M low air loss bed the patient lies on a mattress formed by
five groups of air sacs, adjustable in each section to different air pressure and made of
material permeable to water-vapour. This prevents the formation of pressure sores and
ensures that the patient's skin is kept dry in a comfortable and controlled warm air
atmosphere. In cases of severe burns the patient can be nursed supine for long periods
without being turned and there is no friction against painful burn wounds. When skin
grafts are applied, the patient may be placed on the bed resting on the grafts without
significant damage. The bed can be easily positioned in order to achieve maximum patient
comfort and it can be adapted to accommodate any medical emergency. The recent experiences
with two low air loss beds in the care of burn patients over a period of six months are
described.
Damage to the skin and soft tissues
following prolonged decubitus of the patient in a conventional bed is known to be caused
by excessive pressure of the skeleton on the soft parts, with values 4-5 times as high as
that of the pressure within the capillaries, which is about 26 mm Hg. If these local
conditions persist, the collapse of the capillaries and the veins leads to functional
circulatory disturbances, at first transitory but later permanent, followed by organic
damage with cutaneous necrosis spreading to the subcutaneous tissue, the fascia, the
muscles and the bones.
Further damage is caused by friction between skin and bedsheet due to gravitational
slipping and by imperfect cutaneous evaporation at the pressure points.
All thesel negative conditions are aggravated in the burn patient, who presents impaired
circulatory function, serious cutaneous damage, with necrosis and fluid losses due to
exudation and evaporation. To obviate these conditions Scales proposed to support the
critical burn patient on an air cushion - as if in levitation - without any physical
membrane, according to the hovercraft principle. In view of the technical problems
deriving from the considerable air loss and of the negative psychological effects induced
by this method in the patient, we used an actual air cushion, covered in material which
reduced air loss and offered a number of important advantages: the Low Air Loss Bed System
(LALBS).
This system is intended to ensure body contact over the largest area possible,
distributing an appropriately low pressure throughout the contact surface and allowing
adequate evaporation at the contact points.
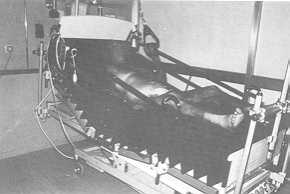
The LALBS model at our Burns Centre (Mediscus Mark 5A-M Bed, Fig. 1) consists of a series
of 21 air sacs made of nylon and microporous polyurethane, impermeable to water but
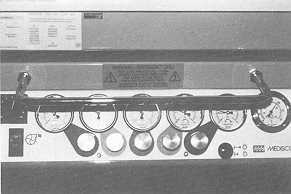
permeable--water-vapour, divided into five groups. Each group is maintained at a selected
pressure and controlled by differently coloured manometers (Fig. 2). The same colours
identify the five sections corresponding to the head, trunk, pelvis, thighs and legs. The
pressure in the sacs can reach 36 cin H 2 0, but does not normally exceced 29 em H 2 0. In
the sections for contact of the lower limbs, the pressure may be as low as half that for
the trunk (Fig. 3).
An electric pump conveys air into the sacs and a system of valves maintains the air at the
desired pressure in each of the five sections. The influx is about 1,400 litres per
minute. The air is heated electrically and thermostatically controlled with a digital
monitor. Air escapes through the lateral seams of the sacs together with water-vapour
emitted by the patient. This continual flow maintains a constant
 |
 |
| Fig. 1:
The Mediscus Mark 5A-M Low Air Loss Bed System. |
Fig. 2:
Control panel at foot of Mark 5A-NI bed with manometers for the 5 air sac sections,
thermometer and digital thermostatic control monitor. |
|
The patient rests directly on the sacs, in
order to avoid alterations of decubital pressure or other undesired complications. In
emergency conditions a sheet, if possible made of the same material as the sacs, is
stretched between the sacs and the patient. Because of their smoothness and fine texture,
the sacs permit easy moving of the patient on the surface of the bed (Fig. 4). Nursing
manoeuvres are facilitated by the capacity of the new model of the LALBS bed to inflate
instantly all the sacs to maximum pressure, thus creating a more rigid and uniform resting
surface for the time required temperature in the patient's immediate environment,
facilitates sterility and keeps the wound and contact surfaces dry.

|
Fig. 3:
Nursing staff checking that air sacs are stretched out and that pressure is not excessive,
in relation to the patient's weight and the body area examined. |
|
Accidental perforation of a sac does not
impair the functioning of the system, which continues to operate also when it is necessary
to remove individual sacs for cleaning. All the sacs are cleaned daily with a 1% Savlon
solution or soap and water. Bacteriological swabs are taken regularly from the sacs in the
various sections and from the filters in the pumping system. Periodically all the sacs are
specially washed at a temperature of 25 'C in a washing-machine, using soap powder, and
then hung up to dry at ambient temperature.
 |
Fig.
4: Movement of the patient on the bed surface is facilitated by the smooth, fine
texture of the sacs and their continuous adaptation to body position. |
|
Another feature of the new model is that
the pumping, heating and control system is mounted directly at the foot of the bed. It is
also now possible to deflate only the section corresponding to the pelvis, making it
easier for the patient to get off and on the bed. All the sacs can be deflated in 5
seconds so that in the event of cardiac arrest resuscitation can be initiated with the
necessary urgency.
Apart from these extreme conditions, the LALBS bed is satisfactory for all the patient's
normal needs, in the various positions and clinical conditions. One electric and two
pneumatic systems make it possible to raise the head and the foot sections of the bed by
up to 30' and the whole support surface can be positioned in Trendelenburg or
anti-Trendelenburg. A control panel enables staff and the patient himself to select the
position preferred: this reduces nursing commitments and greatly increases comfort, as the
burn patient no longer suffers pain at every change of position because of friction
against the bedsheets.
Skin grafts, when applied, can be maintained in position for some days with vaselined
gauzes and thin containing dressings, and then left uncovered, with little risk of trauma
and considerable reduction in the time required for the graft to take and consolidate.
When it is necessary to apply a bandage, the procedure is facilitated by the patient's low
resting pressure, so that it is easy to pass hand and bandage under the burns with minimum
discomfort for the patient. The same holds true for drainage tubes, catheters, etc.
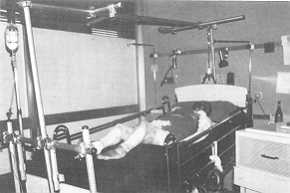
In cases of multiple trauma it is possible to use the orthopaedic traction apparatus
accessory (Fig. 5), with which the two 1ALBS beds in our Centre were fitted some months
ago.
|
Fig. 5: The
orthopaedic traction apparatus accessory fitted to the Mark 5A-NI bed. |
|
RESUME. Le lit LALBS (Low
Air Loss Bed System) à air chaud prévient les plaies de décubitus et permet au patient
brûlé de maintenir les lésions sèches aussi aux points d'appui et de recevoir les
médications sans mouvements douloureux. Dans ces conditions les greffes cutanées
s'attaquent mieux et elles sont moins facilement traumatisées. Il y a un bon niveau de
confort pour le patient et une réduction de l'assistance nécessaire des infirmiers.
BIBLIOGRAPHY
- Leeder CJ.: Use of the low air loss system in
treatment of burns patients. Scand. J. Plast. Reconstr. Surg., 13: 159, 1979.
- Scales J.: Pressure sore prevention. Care Science
Pract., 1: 2, 1982.
- Scales J.T., Lunn H.F., Jeneid P.A., Gillingham
M.E., Redfern S.J.: The prevention and treatment of pressure sores using air-support
systems. Paraplegia, 12: 118, 1974.
- Wyllie F.J., McLean N.R., McGregor J.C.: The problem
of pressure sores in a regional plastic surgery unit. J. Roy. Coll. Surg. Edinb., 29: 38,
1984.
|