Annals of the MBC - vol. 2 - n' 3 -
September 1989
EMERGENCIES:
REGIONAL APPROACHES TO GLOBAL PROBLEMS
Gunn S.W.A.
President, Mediterranean Burns Club
Vice-President, European Centre for Disaster Medicine
SUMMARY. Generalized global
planning in the field of disasters may be remote from regional realities. Two examples of
organizations responsible for successful regional endeavours are the European Centre for
Disaster Medicine, and the Mediterranean Burns Club, both of which emphasize training and
believe in three main principles: a) efTective disaster management requires technical
training; b) such training must be interdisciplinary; c) results are better when there is
maximum common interest. An analysis is made of various principles concerning the
scientific and technical basis of disaster management. It is pointed out that each
disaster has its own epidemiological and pathological profile. Rescue studies show that
immediate rescue is paramount - external help often arrives too late. This emphasizes the
need to educate the general public. Training is necessary, as promoted by the European
Centre for Disaster Medicine, in order to promote the prevention and mitigation of the
effects of disasters through research, training courses, publishing and international
cooperation. The Mediterranean Burns Club offers a specific surgical approach to the
problem. The international community must have mechanisms for planning, mobilization and
co~ordination in order to achieve maximum results. It has however been found that the
action of the various international organizations is more efficient and etTective when
organized and applied on a regional basis.
It is a pleasure for me to appear at this
final session of what has been a very successful attack on disasters.
It may surprise some of you that, for this closing plenary, an international global
conference like EMERGENCY 88 should focus on regional solutions. For both Mr.
Paolini of the European Community and I will look at global problems from the regional
angle.
It is becoming increasingly evident that blanket remedies and global planning, while
applicable in certain circumstances, are proving too dilute and too distant from country
or regional realities, and that the more focussed approaches are proving more productive
and realistic. By "regional" I mean a certain geographic area which, while
diverse in several aspects, such as ethnic composition, shares economic, geographic,
cultural and other affinities, which give it a certain, unity or regional characteristic.
The Mediterranean Basin is such a region. Europe is a larger one, the Caribbean is
another, etc.
The UN, the global Organization par excellence, acts through its Regional Commissions, and
of course the WHO, with which I have long been associated as Head of the Emergency Relief
Operations, is the most successful example of a worldwide but regionalized structure, with
its 6 quasi -independent Regional Offices in Copenhagen, Brazzaville, New Delhi, Manila,
Washington and Alexandria, each with its Emergency Response facility. Geneva is only the
global coordinating Headquarters.
1 shall therefore base my talk on what 1 think to he successful regional endeavours. 1
hope you will forgive me for giving personalized examples - but 1 believe 1 should base
myself on personal experience. 1 refer to the European Centre for Disaster Medicine in San
Marino, of which 1 am Scientific Co-ordinator, and the Mediterranean Burns Club in
Palermo, of which 1 have the honour to be the President.
Both of these organizations emphasize training and are based on three postulates:
- that to be effective, disaster management needs a solid
technical underpinning and a solid basis;
- that training for such action must have an
interdisciplinary-integrated approach; and
- that results are more easily and better achieved when there
is a maximum regional commonality of the problems, the participants and the responses.
1. Scientific and technical
basis of disaster management
Ten principles:
Recent research and field surveys have
shed new light on the effects of natural disaster and have indicated better ways of
providing the appropriate response and needed emergency care. From these technical studies
I would single out the following 10 principles:
- Preparedness is possible. The greater the preparedness for
probable or foreseeable events, the more effective relief operations will be.
- Prevention of many natural disasters is also possible.
- No two disasters are alike, but the problems that a certain
kind of disaster is likely to create are quite foreseeable. Disasters have profiles.
- Based on such profiles, the disease pattern of each kind of
disaster can be formulated epidemiologically.
- Planning and preparedness on a sectorial and international
basis are possible and essential for effective action.
- Mobilization of the appropriate manpower resources in this
case doctors, nurses, nutritionists, primary health care workers - must be so organized as
to be able to respond immediately to the probable and particular needs when disaster
strikes.
- Risk assessment, evaluation of the risks and effects of the
intervention, and a study of the post-disaster situation are essential.
- The post-emergency phase offers an opportunity for taking
steps to mitigate the effects of a subsequent disaster.
- The reconstruction phase starts at once.
- Disaster management takes into full account the community
and the local/national institutions involved.
Total disaster management needs sectorial
research, teaching, training, field experience, community participation, and a workable
cooperative network. Disaster management has now reached a certain degree of maturity, and
I should like to submit that Civil Defence has now become almost a specialty. In any case
there is no place for amateurism. And voluntarism does not mean amateurism.
Disaster profiles
Our surveys have shown that each kind
of disaster has its own epidemiological profile and pathological characteristics, and
these similarities and differences are very important in planning, in prevention and in
relief operations. These studies have indicated new avenues for action and have helped
dethrone many an entrenched myth.
The consequences of a disaster can be immediate, or secondary, delayed, and these differ
with each type of disaster. This applies equally to medical disasters for we know now the
similarities and differences of disease following floods, drought, earthquakes, etc,
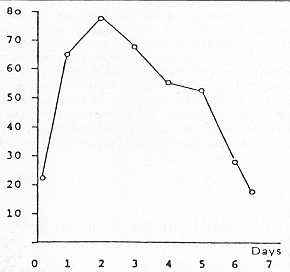
Take hospital admissions following an earthquake - assuming that hospitals have escaped
damage, there will be a rush of in-patient and out-patient arrivals. We now know that once
the rush is over, admission patterns revert to normal as early as the 4th - 5th day after
the earthquake, as shown in these figures from Guatemala.
Rescue studies shed further light
Immediate rescue is paramountl and it
is important to note that any help coming from outside the region almost invariably
arrives too late. Expatriate teams and foreign donors should fashion their assistance
accordingly, if they are to be of any effect. Again in order to maximize local help, it
must be realized that in extracting the trapped and the injured, 90% of the first helpers
come from the village, and 76.2% from the inhabitants of the,,same building. Extraction
with unsophisticated means - hands, shovels, ladder - account for the largest 'number
rescued (96.8%), as opposed to the use of sophisticated measures, such as tractors or
cranes (3.2%). Even the country or the regional neighbours will be too late. Here what
counts is community response. And here is where education of the public finds its shining
place.
Structural patterns
I was saying that disaster management
should be multidisciplinary. Here is an example from the engineering and construction
industries: the relation between the number of storeys of a building and the number of
victims in an earthquake.
These examples that I have chosen are not the expressions of haphazard decisions or
quality judgements. They are based on quantified, objective studies and research, and it
is my plea that more of this kind of scientific work is necessary if our emergency action
is to be of any meaning. To do this, we need basic studies, applied studies, epidemiology,
training courses, teachers, trained personnel.
My second example will address this question of training.
II. Training
Disasters are becoming more frequent,
more serious and more deadly. 1 think 1 have sufficiently shown the need for studies and
training in this field. Within the United Nations several agencies, such as ICDO, are
conducting training courses and UNDRO has been bringing its share to this endeavour. 1
think we have been reasonably successful in getting some institutions to introduce higher
studies in this sector.
As an example let me cite the European Centre for Disaster Medicine, with which, after
many years at WHO, 1 am currently associated. CEMEC is an intergovernmental venture, under
the aegis of the Council of Europe, and housed in the Republic of San Marino. Its aim is
to promote the prevention and mitigation of the effects of natural and technological
disasters through research, investigations, training courses, publishing and international
cooperation. The same applies to the Mediterranean Burns Club, dealing with the surgical
approach to a civil defence problem. It is my conviction that it is through this kind of
approach that we shall be able to make disaster relief more effective.
III. International aid
Following a disaster, international
relief is expected and often provided generously. The international community must
therefore have its mechanism for planning, mobilization and co-ordination, in order to
maximize the effort - an effort that comes from numerous sectors, such as civil defence,
transport, meteorologists, communications, etc.
Generally speaking, four different systems are involved in international assistance -
historically most of the m- born of a disaster - to alleviate disaster. The ICRC was born
on the battlefield of Solferino, the European Community after centuries of conflict, the
United Nations after the Second World War, Oxfam following the famines in Bangladesh, etc.
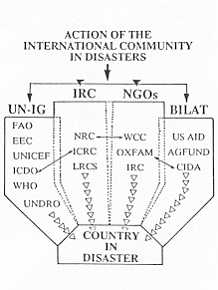
1 think it is worth recalling the make-up of the international aid community. The
following diagram shows the four principal mechanisms of international aid: (1) the
inter-governmental organizations, (2) Red Cross, (3) the NG0s, and (4) direct bilateral
assistance.
This is the pattern of involvement of the international aid and donor community. But
however international these organizations may be, it has been found that their action is
more efficient and more effective when organized and applied on a manageable, regional
basis.
RÉSUMÉ. La planification
globale généralisée dans le camp des désastres peut sembler loin des réalités
regionales. Il existent deux examples d'organisations responsables d'initiatives
régionales réussies; le Centre Européen de la Médecine des Désastres, et le Club
Méditerranéen des Brûlures. Tous les deux soulignent l'importance de la formation
professionnelle et ils croient en trois principes fondamentaux: a) la gestion efficace des
désastres requiert une formation technique; b) cette formation doit être
interdisciplinaire; c) les résultats sont plus favorables quand il y a le maximum
d'interêt commun.
L'auteur analyse les différents principes de la gestion des désastres. Il relève que
chaque désastre a un profil épidémiologique et pathologique propre. Les études des
secours montrent que le secours immédiat est de la plus haute importance - le secours qui
vient d'ailleurs arrive souvent en retard. Cela souligne l'importance d'éduquer le grand
public. La formation professionnelle est necessaire, comme elle est promue par la Centre
Européen de la Médecine des Désastres, pour promouvoir la prévention et la réduction
des effets des désastres à travers la recherche, les stages, les publications et la
coopération internationelle. Le Club Méditerranéen des Brûlures offre une approche
chirurgicale spécifique au problème. La communauté internationale doi - t avoir des
mécanismes pour la planification, la mobilisation et la coordination pour arriver aux
résultats maximums. On a cependant trouvé que l'action des différentes organisations
internationales est plus efficiente et plus efficace quand elle est organisée et
appliquée sur base régionale.
BIBLIOGRAPHY
- Assar M.M.: "Guide to sanitation in natural
disasters". Geneva, World Health Organization, 1971.
- Clarke R., Ehrlich A., Gunn S.W.A. et al.:
"London under attack". Report of the GLAWARS Commission. Oxford and New York,
Blackwell, 1986.
- De Bruyeker M., Greco D., Lechat M. et al.: The 1980
earthquake in southern Italy. Bull. Wld Hlth Org., 61: 102n 1983.
- Gunn S.W.A.: Disaster medicine and emergencies. J.
Irish Coll. Phys. & Surg., 17: 14, 1988.
- Gunn S.W.A.: Medical management in international
relief, UNDRO News, pp. 8-24, Sep. 1987.
- Gunn S.W.A.: Multilingual dictionary of disaster
medicine and international relief. Dordrecht, Kluwer Academic Publishers, 1989.
- Jeannet E.: "Catastrophes et m6decine".
Lausanne, Payot, 1985.
- UNDRO: Prevention and mitigation of disasters:
Sanitary aspects. United Nations, Geneva and New York, 1982.
|