Annals of the MBC - vol. 2 - n' 3 -
September 1989
A PROPOSAL FOR THE
STRATEGIC PLANNING OF MEDICAL SERVICES IN THE CASE OF MAJOR FIRE DISASTERS IN THE CITY OF
BARI
Dioguardi R, Brienza E, Portincasa A., Di Lonardo A.,
Matarrese V.,
Cattedra di Chirurgia Plastica e Ricostruttiva, Universita
degli studi di Bari, Italia
SUMMARY. In
view of the high level of industrialization in the City of Bari and the consequently large
work-force, we considered it imperative to define a health strategy to be followed in the
event of a fire disaster. The contents of this paper are part of a planning proposal
presented to the different authorities in charge of managing the city and surrounding
territory (Prefecture, Military Authorities, Town Council, Fire Brigade). As said, our
objective was to identify, in the light of experience gained in other cities, potentially
critical areas in the city, and in particular:
1) the industrial zone (the site of a thermoelectric power plant and oil refineries);
2) the railway stations;
3) the port area (with crude oil stocks).
We have also identified the main routes into and out of the city, transit routes for
rescue vehicles, and prepared a thorough organizational plan. This strategy, which we are
sure can only be successful with the intervention and control of the Armed Forces,
proposes the following four phases of development:
* Alarm phase: by appropriate means of communication;
* Organizational phase: selection of a coordination centre;
• Activation phase: selection of three distinct operative areas plus field hospital;
• Specialist health treatment phase: Plastic surgery, burns surgery.
In view of the ever more industrialized
nature of Bari in recent years, we feel there is an urgent need to define a strategy for
deploying the medical services to be relied on in the case of a major fire disaster.
In our opinion, an emergency situation requiring the treatment of a large number of
severely burned patients, and creating consequent organizational needs as regards first
aid, transport and hospitalization, can be caused by two possible occurrences:
- a foreseeable disaster
- an unforeseeable disaster.
A foreseeable disaster can be defined as
an accident which could occur in an industrial district in Bari with a high fire risk. For
such an occurrence, a pre-established plan of operations could be drawn up.
It therefore seems of fundamental importance to identify those areas in Bari which could
be defined as being at high risk.
Analysis reveals that four areas can be considered at high risk:
- the industrial area (containing a thermoelectric power
station and oil refineries)
- the railway stations
- the area around the port and the 'Fiera del Levante'
exhibition grounds (containing unrefined oil tanks)
- the area around the airport.
In these areas highly flammable materials
are concentrated in high quantities with respect to the surface area, thus constituting
critical zones with a high fire risk.
An unforeseeable catastrophe includes all those accidents for which, owing to the expected
nature of their development, a pre-established plan cannot be drawn up.
However, in this case too, a general plan, derived from those drawn up for foreseeable
disasters and modified according to need, could be used.
In drawing up an organizational plan for use in the case of disaster, some parameters must
be carefully considered: the number of victims, the type of lesions, the difficulties
posed by the limited number of vehicles available for transporting to and from the
disaster area, the lack of hospital beds, the small number of burn units.
These conditions make it vital to pre-establish a programme of assistance in order to
avoid loss of time, confusions, error and overlapping of responsibilities.
The considerations in our study are part of a planning proposal presented to the
appropriate authorities of the city and its territory (Prefecture, Military Authorities,
Local Council, Fire Brigade).
A plan for the organization of medical assistance in emergencies cannot be drawn up
without a multi-centre collaboration. The medical administration should be entrusted to
those who face these emergencies every day: a multidisciplinary team including both burn
and intensive care specialists seems to us the best solution.
After consultation with the centres collaborating in the plan of assistance, the
coordinator of the medical assistance should set up operational centres.
Operational centres
O.C.1) Field Hospital;
O.C.2) Burn Centre in the city;
O.C.3) Hospitals in the Province of Bari (with/without Plastic Surgery Dept.);
O.C.4) other Bum Centres in Italy.
Triage
Before detailing each component's
tasks and the development of the various phases of assistance, a fundamental problem in
disaster emergencies should be considered: triage, or classification of the wounded
according to the clinical conditions. In fact, it is better to divide the patients under
observation into classes:
1st class: deceased
2nd class: injured with life-threatening problems
3rd class: severely injured needing immediate care and/or surgical intervention within a
short time
4th class: less severely injured who can be discharged after first aid.
These classes, distinguished by colour, enable the real
severity and the suitable destination of the patients to be defined.
Ist class: black
2nd class: red
3rd class: yellow
4th class: green.
The deceased must be transferred immediately to the city
morgues, away from the areas destined for assistance and medication.
The injured of the 2nd and 3rd classes must be transported to the primary centre where,
after restoration of vital functions, transferral to alternative operational centres can
be decided on. The injured of the 4th class are medicated on site and discharged.
The institution of a field hospital (primary operational centre) seems to us extremely
important. Its rapid creation and prompt availability enables the situation to be kept
under control during the first 24-48 hours (the period in which the condition of the
severely burned patient is very delicate), and triage can be carried out.
It is also important to define the principal access and escape routes and the transit
roads for ambulances etc. A precise plan defining the various areas of responsibility and
competence is an absolute necessity.
A strategy of intervention on these lines cannot succeed without the help of the Armed
Forces. Thus an Emergency Intervention Group (E.I.G.), classified by colour, must be
constituted as follows:
1) green: the elements in this group go into action at the time of the disaster, with the
task of removing the cause
- Fire Brigade
- Civil Defence Ministry - Armed Forces
- blue: this group is in charge of regulating the traffic on
the access and escape routes, and if necessary of evacuating the zone around the area of
the disaster - Municipal Police - State Police - Carabinieri red: this group is in charge
of activating the strategic plan for the medical services
- multidisciplinary medical team (burn and resuscitation
specialists)
- Italian Red Cross
- Ser-Bari (Voluntary Ambulance Service).
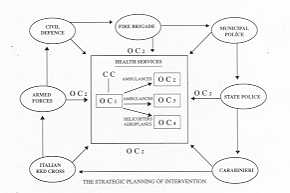
The plan of intervention
The plan develops over four phases: - alarm phase -
organizational phase - activation phase - specialist intervention phase.
The Alarin Phase
From the moment of the
"alarm", transmitted directly by telephone or the local communication system, or
indirectly by the inhabitants of the area around the disaster, amateur radio transmitters,
etc. ' the mobilization of the E.I.G. should occur within l0-30 minutes.
The scheme in Fig. 1, activated by each group of assistance and developing in a clockwise
direction, shows the various responsibilities involved in this phase.
A previously agreed formula of the type:
"This is an emergency. Absolute priority emergency" should be used over the
telephone, to avoid misunderstanding.
The Organizational Phase
The Coordination Centre (C.C.) is
defined in this phase. The C.C. is instituted in the immediate vicinity of the field
hospital, and is in charge of the entire organization of the plan of intervention. This
task is entrusted to the Military Authorities and is activated within 20-40 minutes:
sufficient time to trigger off the medical plan.
The Activation Phase
The strategic medical plan is put into
effect during this phase, and the primary operational centre OCI and secondary operational
centres (OC2, OC3, OC4) are defined.
The institution of the OCI field hospital and the C.C. in the vicinity of the disaster is
of vital importance both for the preliminary triage and for the immediate care of the
injured in the 3rd and 4th classes.
An operation of this type should make the OCI available within 30-50 minutes.
The Specialist Intervention Phase
This phase begins with the
intervention of the burn and intensive care specialists and continues beyond the first
24-48 hours when the transferral of patients to the secondary operational centres for
intensive care and surgery has been determined. This phase has an undefined duration.
Conclusions
Although this proposal does not claim
to provide an answer to all the problems which could arise, particularly in the case of
unforeseeable disasters, it nevertheless seems to be a possible solution if the disaster
occurs in the areas we have identified as potentially at high risk.
In view of the traffic situation in Bari, careful consideration should be given to the
details of the proposal, particularly as regards the routes to and from the site of the
catastrophe. Obviously a sense of discipline and commitment beyond normal duties in all
concerned is vital.
Naturally an occurrence such as a major fire disaster involving a large number of victims
requires that each single operator be aware of the special demands an emergency situation
inevitably creates ("emergency mentality").
The importance of the role of the Armed Forces, by their nature most fitted for coping
with emergencies, must be stressed in organizing every detail of the plan of assistance:
- triggering off the alarm phase , by communicating
immediately with the members of the E.I.G. to be mobilized
- evacuating the areas surrounding the site of the disaster
and creating a clear thoroughfare for the passage of all forces involved in the plan of
assistance
- defining and instituting the Coordination Centre and Field
Hospital to guarantee the immediacy of the first phase of the plan
- contacting the secondary Operational Centres (Burn Unit in
the city, Regional Hospitals, other Burn Units in Italy)
- arranging for an adequate number of vehicles (ambulances
and aircraft) to be available
- transporting the injured to the primary Operational Centre.
Although we do not consider Medicine in
Disasters to be qualitatively different from daily medical urgencies (but rather a
concentration in time and space of events which occur widely every day), a proposal for a
strategic medical plan in the case of a fire disaster in Barl seemed to us opportune. We
also feel that a plan of this type could be adapted to other disaster situations not
caused by fire and occurring in other areas.
We have tried to avoid theoretically perfect but inapplicable plans, concentrating on a
simple and practical scheme, working systematically and attributing at each stage the
responsibilities of the groups involved in order to adopt the most correct approach
towards the Whilst an emergency department directed by an Intensive Care Unit, including
neuro-, thoracic, emergency and plastic surgery and orthopaedics, would certainly be
useful, we believe that in a catastrophe of this type a bidisciplinary medical team
consisting of burn and intensive care specialists will suflice to manage the emergency
intervention plan, if t e latter is, as in this case, previously organized in every
detail.
RÉSUMÉ. En considération du
niveau élevé d'industrialisation dans la cité de Bari et de la main-d'oeuvre en
conséquence très nombreuse, nous avons voulu définir une stratégie sanitaire à suivre
en cas d'incendie désastreux. Le contenu de cet article fait part d'une proposition de
planification présentée aux différentes Autorités responsables de la gestion de la
cité et du territoire environnant (Préfecture, Autorités Militaires, Conseil Municipal,
Corps des Pompiers). Notre but était d'identifier, à la lumière d'expérience acquise
en d'autres cités, les zones potentiellement critiques, et en particulier: 1) la zone
industrielle (le site d'une centrale thermoélectrique et de raffineries de pétrole), 2)
les gares; 3) la zone du port (avec dépôts de pétrole brut). Nous avons identifié les
routes principales d'entrée et de sortie de la cité et les routes de passage pour les
moyens de secours; nous avons aussi préparé un plan exhaustif d'organisation. Cette
stratégie, qui peut réussir seulement à notre avis avec le soutien des Forces Armées,
propose quatre phases de dévéloppement:
- • Phase d'alarme: par les moyens de
communication plus indiqués;
- • Phase d'organisation: sélection d'un centre
de coordination;
- • Phase de secours: sélection de trois zones
opérationnelles distinctes plus hôpital de campagne;
- • Phase de thérapie sanitaire spécialiste:
chirurgie plastique, chirurgie des brûlures.
BIBLIOGRAPHY
- Finch F., Nancekievill D.C.: The role of hospital
medicals at a major accident. Anest 30: 666-676, 1975.
- Montaigne: I would have everie man write what he
knowes and no more. Brit. J. of Anest, 48: 6, 1976.
- Arturson G.: The los Alfaques Disaster: a
boiling-liquid, expand i ng-vapour explosion. Burns, 7: 233-251, 1981.
- Konigova R., PoIndelicek I.: Psychology associated
with mass burn disasters. Burns, 8: 64-66, 1982.
- Finch P.M., Hamilton T.: Early documentation of
disaster victims. Anest, 37: 1185-1189, 1982.
- Caro D.H.J.: Strategic planning of burn care
services and role of information systems. Burns, 8: 227-230, 1982.
- Bozza, Marrubini et al.: Classification and triage
of burn injuries, 3rd World Cong. on Ernergency-Disaster Med., 413, 1983.
- Campos C.: La reponsabilidad social ante las
catastrofes. Rev. Espan. Anest. Rean., 31: 3, 1984.
- Das R.A.P.: 1981 Circus fire diaster in Bangalore,
India: Causes, management of burn patients and possible presentation. Burns, 10: 17-29,
1984.
- Glasheen W.P. et al.: Evaluation of an emergency
medical service referral system for burn patients. Burns, 10: 323-330, 1984.
- Moxon M.A.: Fire in the operating theatre.
Evacuation pre-planning may save lives. Anest, 41: 543-546, 1986.
- Morra et al.: Piano di emergenza di un Ospedale
zonale in caso di catastrofe. Minerva Anest, 52: 1986.
- Arturson G.: The tragedy of San Juanico-the most
severe LPG disaster in history. Burns, 13: 87-102, 1987.
|