Annals of the MBC - vol. 2 - n* 4 -
December 1989
EXTENSIVE BURN
PATIENTS: IMMUNOLOGICAL PROBLEMS
Visentini P.
Divisione di Chirurgia Plastica e Centro Ustioni
dell'ospedale Civile di Udine, Italia
SUMMARY.
The bum lesion provokes immune depression, which favours bacterial aggression. This was
documented in our laboratory by examining the values of gammoglobulin and T lymphocytes in
the blood. General and local treatment for the reduction of the depression of the
immunocompetent cells is described, together with results of the monitoring of T3, T4 and
T8 lymphocytes. It was observed that the reduction of these immunocompetent cells was
evident in extensive bum patients, elderly patients, and those with full-thickness bums.
An attempt was made in 72 patients to counteract the reduction of T lymphocytes using
thymostimulin (TPI), regulating dosage on the basis of the monitoring of the absolute
value of the lymphocytes. With this treatment there was a reduction in infections and
improvement in survival, especially in elderly patients and those with full-thickness
bums.
The bum patient frequently presents immune
system depression which is indicated by:
- the observation that homologous cutis grafts are eliminated
after a longer time period than in other patients;
- the reduction of gammoglobulins;
- the often considerable reduction of T lymphocytes,
particularly of T4 lymphocytes.
These modifications could be correlated to
the difficulties the bum patient has in defending himself from bacterial aggression.
We therefore decided to document this difficulty by monitoring some parameters such as the
gammoglobulin rate and the absolute number of T3, T4 and T8 lymphocytes. Our
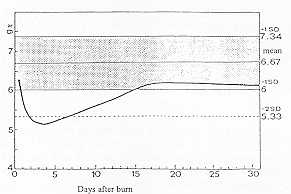
experience, as shown in Fig. 1, indicates that the burn patient presents a reduction of
total proteins, which we determined in 160 patients with 2nd or 3rd degree burns in 10-95%
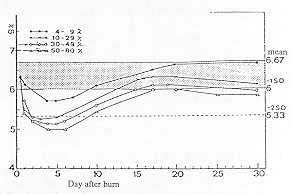
BSA, average 29%. The drop in total proteins, as can be seen in Fig. 2, is proportional to
the burn surface area.
The determination of T lymphocytes
demonstrated that the reduction was more marked in elderly patients, in extensive bum
patients and in those with full-thickness bums. In some cases the values measured were
similar to those seen in AIDS cases. The condition persisted during the acute phase of the
disease and regressed as the patient's health gradually improved.
According to data in the literature, depression of the immunocompetent cells is increased
by associated trauma, catheters, insufficient introduction of alimentation, viral and
bacterial infections, diabetes mellitus, hepatic cirrhosis, blood transfusions and a
number of drugs, such as analgesic-antipyretics derived from pyramidone, corticosteroids,
etc. Immune depresion can be controlled in many ways -by an infusive treatment that
maintains the protein composition of the blood at about normal values, especially albumin
and gammaglobulin, by adequate introduction of alimentation, either orally, parenterally
or by naso-gastric tube, by a local and general treatment that reduces infective processes
as far as possible, and if necessary by the administration of drugs that stimulate the
production of immunocompetent cells. For many years we have treated extensive burn
patients from the beginning with human plasma (isogroup, if possible) using the formula we
have elaborated (Formula N' 1) for the first 2 days, in order to maintain normal
haematocrit values. Fig. 3 - Mean values of protein fractions separable by
electro-phoresis, determined in burn patients with lesions of 10-95%. Comparison with mean
control values +/Standard Deviation.
We also correct gammoglobulin values. The necessary electrolyte solutions are administered
from the beginning. We also administer cimetidine, to prevent gastric stress ulcer, and
calciparin in elderly-, and very extensive bum patients, to reduce the risk of pulmonary
embolisms. Antibacterial drugs are administered in the presence of signs of infection like
fever or a considerable increase in leucocytes, the choice being based on the
antibiograms. Alimentatioft is systematically controlled so that the necessary calories
are introduced.
Last of all, let us consider the surgical operation, which as early as possible must
remove necrotic tissue and replace it with autologous grafts. This is unfortunately
possible only in patients with burns of modest extent - in extensive burned patients early
treatment is possible only in the face and hands. However all the above procedures
are sometimes unable to prevent the reduction in particular cases of the immunocompetent
cells, which we a4so have observed, determining systematically the absolute number of T3,
T4 and T8 lymphocytes (CD3, CD4, C138).
72 patients of varying age and with different extent and depth of lesion, presenting a
marked reduction of immunocompetent cells, were treated with thymostimulin (TPI)*,
regulating the dosage on the basis of the monitoring of T lymphocytes. In particular, when
the number of immunocompetent cells presented a reduction of at least 20%, we administered
I mg/kg of TPI for 7 days. When the reduction of immunocompetent cells was higher, in some
cases even 60%, we administered 1.5 mg/kg, also for 7 days.
When the immunocompetent cells returned to near normal values we administered TPI at the
rat~ of I mg/kg once or twice a week. We were ready to resume daily administration in the
event of reduction of the immunocompetent cells, which generally occurs following surgical
operation.
For over a year, before serious operations, we have initiated daily treatment, which we
suspend when the immunocompetent cells reach normal values.
As said, the 72 patients treated presented burns of various extent and depth and were of
varying age (see Tables). Some with bums in the upper airways had to be tracheotomized;
others also had traumas and fractures. The elderly patients often suffered from
cardiopathies, diabetes and arteriosclerosis; one patients had AIDS and some were
alcoholics or drug addicts with hepatic damage.
In all patients treated with TPI we observed a reduction of bacterial aggression, a lower
drop in gammaglobulins, less need to administer antibiotics, favourable progress and the
possibility of early operation even in extensive burn patients.
As these data are not easy to document objectively, we have calculated the mortality rate
comparing it with that reported in Feller and Crane's Table (Table 1) and with bum
patients we treated in previous years (Table 2).
Table 3 refers to 72 patients of varying age and with different extent and depth of
lesions treated with TPI in the way described. They present a survival rate of 93.05%,
compared to a rate of 82.27% according to Feller and Crane and 90.47% according to
Visentim et al.
Table 4 refers to 49 patients with bums of varying extent and depth, aged up to 59 years,
treated with TPI. They present a survival rate of 93.87% compared to 87.22% according to
Feller and Crane and 94.12% according to Visentini et al. One of the deceased was HIV
positive.
% BURN AREA |
AGE |
TOTAL |
| 0-1 |
2-4 |
5 -9 |
10-19 |
20-39 |
40-59 |
60- 100 |
| 0-9 |
100 |
100 |
100 |
100 |
100 |
97 |
91 |
99 |
| 10-19 |
99 |
99 |
100 |
100 |
100 |
97 |
73 |
97 |
| 20-29 |
94 |
95 |
99 |
99 |
98 |
90 |
46 |
93 |
| 30-39 |
71 |
81 |
85 |
96 |
92 |
66 |
13 |
81 |
| 40-49 |
48 |
66 |
80 |
86 |
80 |
51 |
9 |
69 |
| 50-59 |
18 |
44 |
52 |
76 |
69 |
22 |
9 |
51 |
| 60-69 |
0 |
19 |
42 |
50 |
48 |
33 |
4 |
36 |
| 70-79 |
29 |
7 |
25 |
25 |
23 |
8 |
0 |
18 |
| 80-89 |
0 |
7 |
25 |
22 |
13 |
8 |
0 |
10 |
| 90- 100 |
0 |
11 |
0 |
13 |
2 |
0 |
0 |
3 |
| TOTAL |
91 |
89 |
90 |
90 |
86 |
75 |
51 |
84 |
|
Table I -
ANALYSIS OF MORTALITY. PERCENTAGE OF SURVIVAL IN RELATION TO AGE AND BSA |
|
| % BSA |
N'
Patients |
Survival
rate according
to Feller and
Crane |
Survival rate
according to
Visentini
et al. |
N* of
survivors |
| 0- 9 |
24 |
22.80 |
23.88 |
24 |
| 10-19 |
18 |
16.25 |
16.80 |
18 |
| 20-29 |
13 |
11.26 |
11.20 |
11 |
| 30-39 |
6 |
3.58 |
5.66 |
6 |
| 40-49 |
8 |
4.40 |
6.40 |
6 |
| 50-59 |
1 |
0.69 |
0.87 |
1 |
| 60-69 |
- |
- |
- |
- |
| 70-79 |
- |
- |
- |
- |
| 80-89 |
1 |
0.13 |
0.33 |
1 |
| 90- 100 |
1 |
0.13 |
0.00 |
0 |
| TOTAL |
72 |
59.24 |
65.54 |
67 |
| % SURVIVAL |
|
82.27% |
90.47% |
93.05% |
|
| Table 3 PATIENTS WITH
FULL-THICKNESS BURNS TREATED WITH TP1. COMPARISON BETWEEN FELLER AND CRANE'S TABLE (7,508
PATIENTS), 1970 AND OF VISENTINI ET AL. (N' PATIENTS 933), 1987 |
|
| % BSA |
N'
Patients |
Survival
rate according
to Feller and
Crane |
Survival rate
according to
Visentini
et al. |
N* of
survivors |
| 0- 9 |
12 |
11.88 |
12.00 |
12 |
| 10-19 |
12 |
11.88 |
12.00 |
12 |
| 20-29 |
11 |
10.34 |
9.92 |
10 |
| 30-39 |
5 |
3.50 |
5.00 |
5 |
| 40-49 |
6 |
4.22 |
6.00 |
5 |
| 50-59 |
1 |
0.69 |
0.87 |
1 |
| 60-69 |
- |
- |
- |
- |
| 70-79 |
- |
- |
- |
- |
| 80-89 |
1 |
0.13 |
0.33 |
1 |
| 90-100 |
1 |
0.13 |
0.00 |
0 |
| TOTAL |
49 |
42.74 |
46.12 |
46 |
| % SURVIVAL |
|
87.22% |
94.12% |
93.87%
(95.91%) |
|
Table 4
PATIENTS WITH FULL-THICKNESS BURNS AGED BETWEEN 0 AND 59 YEARS TREATED WITH TP1.
COMPARISON BETWEEN FELLER AND CRANE'S TABLE (7,508 PATIENTS), 1970 AND THE TABLE PREPARED
BY VISENTINI ET AL. (N' PATIENTS 933), 1987 |
|
Feller and Crane's table
Table 5 refers to 23 patients with
full-thickness skin bums aged over 60 years treated with TPI. The survival rate was 91.30%
against 71.82% according to Feller and Crane and 82.69% according to Visentini et al.
Table 6 (Feller and Crane) analyses survival rate on the basis of extent and age,
considering only full-thickness bums.
Table 7 shows the reduction of mortality, which is very evident, calculating only
full-thickness bums in 60 patients treated with TPI. We obtained a survival rate of 93.33%
compared to an estimated rate (Feller and Crane) of 71.28%.
The summary table (Table 8) shows that the survival of bum patients treated with TPI
administered regulating the amount on the basis of the monitoring of the T cells is very
low in young patients, good in elderly patients and very high in bum patients with deep
bums.
The techniques currently employed make it possible to cure a high number of patients with
extensive and complicated bums, even in elderly patients.
In many cases however the quality of the cure IS not perfect, and 1 think that this is a
very important field of research for our younger colleagues.
(*) Thymostimulin - TP1 - produced by Seronno was used
| % BSA |
N'
Patients |
Survival
rate according
to Feller and
Crane |
Survival rate
according to
Visentini
et al. |
N* of
survivors |
| 0- 9 |
12 |
10.92 |
11.88 |
12 |
| 10-19 |
6 |
4.38 |
4.80 |
6 |
| 20-29 |
2 |
0.91 |
1.28 |
1 |
| 30-39 |
1 |
0.13 |
0.66 |
1 |
| 40-49 |
2 |
0.18 |
0.40 |
1 |
| 50-59 |
- |
- |
- |
- |
| 60-69 |
- |
- |
- |
- |
| 70-79 |
- |
- |
- |
- |
| 80-89 |
- |
- |
- |
- |
| 90-100 |
- |
- |
- |
- |
| TOTAL |
23 |
16.52 |
19.02 |
21 |
| % SURVIVAL |
|
71.82% |
82.69% |
91.30% |
|
Table 5
PATIENTS WITH FULL-THICKNESS BURNS AGED BETWEEN 60 AND 90 YEARS TREATED WITH TP1.
COMPARISON WITH FELLER AND CRANE'S TABLE (7,508 PATIENTS), 1970 AND THE TABLE OF VISENTINI
ET AL. (N' PATIENTS 933), 1987 |
|
%
BURN
AREA |
AGE |
TOTAL |
| 0-1 |
2-4 |
5-9 |
10-19 |
20-39 |
40-59 |
60-100 |
| 0-9 |
97 |
98 |
100 |
99 |
98 |
94 |
83 |
97 |
| 10-19 |
78 |
89 |
95 |
93 |
89 |
85 |
51 |
86 |
| 20 - 29 |
36 |
84 |
87 |
90 |
72 |
57 |
23 |
70 |
| 30-39 |
33 |
67 |
75 |
69 |
60 |
32 |
3 |
53 |
| 40-49 |
20 |
40 |
70 |
58 |
37 |
21 |
6 |
37 |
| 50-59 |
0 |
35 |
38 |
25 |
30 |
7 |
0 |
24 |
| 60-69 |
0 |
6 |
20 |
39 |
10. |
0 |
0 |
9 |
| 70-79 |
0 |
11 |
14 |
11 |
7 |
0 |
0 |
7 |
| 80-89 |
0 |
0 |
16 |
0 |
0 |
0 |
0 |
1 |
| 90-100 |
0 |
0 |
0 |
0 |
5 |
0 |
0 |
2 |
| TOTAL |
91 |
89 |
90 |
90 |
86 |
75 |
51 |
84 |
|
| Table 6 ANALYSIS OF MORTALITY:
SURVIVAL RATE IN RELATION TO AGE AND FULL-THICKNESS BURNS |
|
| % BSA |
N'
Patients |
Survival
rate according
to Feller and
Crane |
N* of
survivors |
| 0- 9 |
29 |
26.12 |
29 |
| 10-19 |
14 |
11.04 |
14 |
| 20-29 |
7 |
3.58 |
6 |
| 30-39 |
3 |
0.67 |
3 |
| 40-49 |
5 |
1.06 |
3 |
| 50-59 |
1 |
0.30 |
1 |
| 60-69 |
- |
- |
- |
| 70-79 |
- |
- |
- |
| 80-89 |
- |
- |
- |
| 90-100 |
- |
- |
- |
| TOTAL |
60 |
42.77 |
56 |
| % SURVIVAL |
|
71.28% |
93.33% |
|
Table 7
BURNS PATIENTS WITH FULL-THICKNESS BURNS TREATED WITH TP1. COMPARISON WITH FELLER
AND CRANE'S TABLE (7,508 PATIENTS), 1970. |
|
RÉSUMÉ. La
réintégration calorique-protéique du brûlé représente un moment thérapeutique très
important parce que la prévention ou la réduction du catabolisme peuvent protéger les
fonctions organiques et réduire la morbidité et la mortalité. Le but principal est la
satisfaction des besoins calorique-protéiques en tentant d'en administrer la quantité
maximum entre 3-4 jours après la brûlure, ce qui déchaîne un mécanisme de freinage
catabolique. Il faut absolument faire une évaluation précise de l'état nutritionnel du
patient au moment de l'hospitalisation et pendant tout le séjour à l'hôpital. A cette
fin on emploie divers paramètres de référence chimiques, biohumoraux,
anthropométriques et immunologiques. Les Auteurs décrivent les divers types de soutien
nutritionnel (Entéral Total, Entéral avec Soutien Parentéral Total) et les tests
relatifs, les indications et les contre-indications.
BIBLIOGRAPHY
- Arturson G.: Computer simulation of fluid
resuscitation in thermal injury. Burns, 14: 257, 1988.
- Barisoni D.: "Le ustioni ed il loro
trattamento", Piccin, 1984.
- Dogo G., Visentini P.: Plasma in anti-shock therapy
of burned patients: clinical findings and considerations. Pharmacological treatment in
bums, Excerpta Medica, 59, 1968.
- E. Echinar C.: Immunity of the burned patient. Scand
J. Plast. Reconstr. Surg., 21: 317, 1987.
- Yong Chih-Chun, Hsu Wei-Shia, Shih Tsi-Siang:
"Treatment of bums", Shanghai Scientific and Technical Publishers,
Springer-Verlag, Berlin, Heidelberg, New York, 1982.
- Soave R.: "Lospite immunocompromesso. Manuale
pratico di malattie infettive", p. 594, Antonio Delfino, 1988.
- Feller 1. Crane K.H.: Ufficio Nazionale (U.S.A.) per
Io scambio di informazioni sulle ustioni. La clinica chirurgica del nord America -
Chirurgia delle ustioni, Vol. 3 n' 6, Picciri, 1978.
- Visentini P. et al.: Modifiche della immunità
celluic -iediata negli interventi di Chirurgia Plastica. Atti del 37' Congresso Nazionale
della Società Italiana di Chirurgia Plastica ricostruttiva ed estetica: p. 1191, 1988.
- Visentini P. et al.: Our experience in treatment of
burned patients. Annals of the NIBC, 1: 107-112, 1988.
- Visentini P.: Considerazioni sulla malattia ustione.
Rivista italiana di Chirurgia Plastica, 2: 121, 1970.
- Visentini P. et al.: La monitorizzazione della
proteinemia nell'ustionato. Rivista Italiana di Chirurgia Plastica, 12: 221, 1980.
|