Annals of the MBC - vol. 2 - n' 4 - December 1989 AN ALGORITHM FOR STANDARIZED CARE AND ASSESSMENT OF HAND BURNSRosenberg L., Shani E., Greber B., Carmel C., Sagi A. Soroka University Hospital & The R&D Center for Plastic Surgery Advanced Services, Israel SUMMARY. The objective assessment of all factors involved in the treatment of hand bums is the indispensable basis of our body of knowledge of the subject, especially knowledge gathered by large numbers of observers and centres with direct or indirect bias. Such critical assessment has to be based on well-defined criteria known to all participating members. The different criteria have to follow a logical sequence based on the entire natural and dynamic course of the pathological and therapeutic process. Such a flow chart of clinical findings, decisions and alternatives forms an algorithm. We present the algorithmic process of hand bums care and assessment of our Centre. The algorithm itself has been successfully implemented in our service. We appeal to other centres to join our efTort of establishing, collecting and editing similar algorithms into a reference manual. 1. Check-list for treatment of hand burns 1. Name: date of birth: I.D.: today's date: date of bum: time of bum: cause of bum: area of bum: CM2 (Total) c:] volar r:i, dorsal [I fingers (Include body surface area burn chart) History of allergy to:
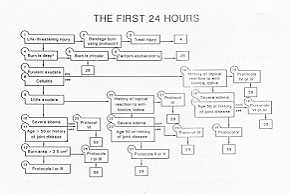
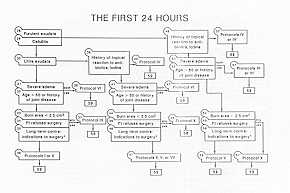
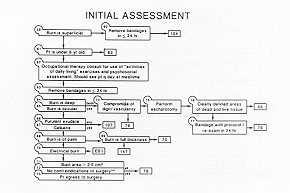
History of joint disease, disease type 2. Initial examination
3. Primary assessment
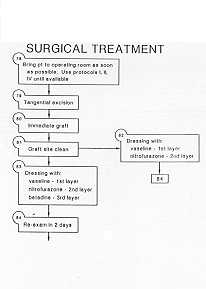
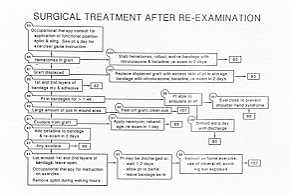
4. Surgical treatment
5. Surgical patient assessment
other complications: treatment including patient instructions: occupational therapy consult next exam planned: (days) 6. Surgical patient discharge
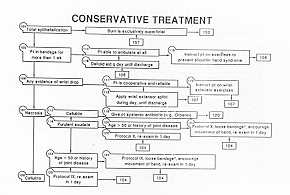
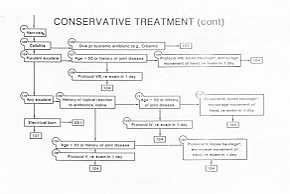
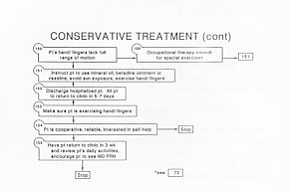
7. Conservative treatment patient assessment
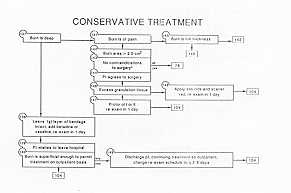
8. Conservative treatment patient discharge
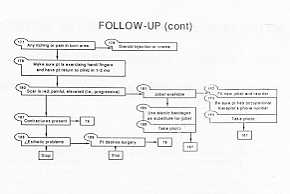
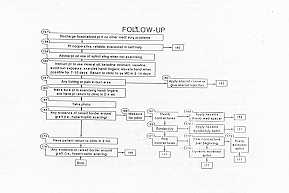
9. Follow-up
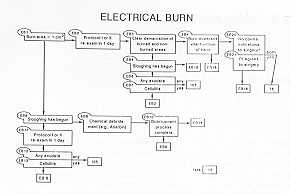
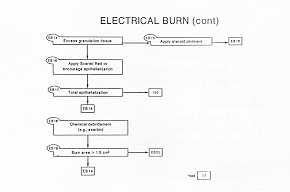
Protocol 1 removal of any blisters cover with nitrofurazone gauze cover with thick absorbent dressing use elastic bandages Protocol 2 removal of any blisters cover with nitroftirazone gauze cover with Betadine-soaked gauze cover with thick absorbent dressing use elastic bandages Protocol 3 open passive dressing Protocol 4/A removal of any blisters cover with nitrofurazone gauze cover with saline-soaked gauze cover with thick absorbent dressing use elastic bandages Protocol 4/B same steps as 4/A use continuous infusion of saline Protocol 5/A removal of any blisters cover with nitrofurazone gauze cover with Betadine- or neomycin-streptomycin soaked gauze cover with thick absorbent dressing use elastic bandages Protocol 5/B same steps as 5/A use continuous infusion of neomycin-streptomycin or Betadine Protocol 6/A removal of any blisters cover with nitrofurazone gauze cover with M9S04 cover with thick absorbent dressing use elastic bandages Protocol 6/B same steps as 6/A use continuous infusion Of M9S04 Protocol 7 removal of any blisters apply silver sulphadiazine to bum use plastic bag covering Protocol 8 removal of any blisters apply silver sulphadiazine to burn cover with thick absorbent dressing use elastic bandages Protocol 9 removal of any blisters apply debridement agents (e.g. Aserbin) cover with thick absorbent dressing use elastic bandages Protocol 10 removal of any blisters apply debridement agents (e.g. Aserbin) apply silver sulphadiazine to bum cover with thick absorbent dressing use elastic bandages
RÉSUMÉ. L'évaluation
objective de tous les facteurs relatifs au traitement des brûlures des mains constitue la
base indispensable pour l'ensemble de nos connaissances du sujet, et en particulier les
connaissances recueillies par un grand nombre d'observateurs et de Centres avec un
intérêt direct ou indirect. Cette évaluation critique doit être basée sur des
critères bien définis reconnus par tous les participants à la recherche. Les
différents critères doivent suivre une séquence logique basée sur tout le cours
naturel et dynamique du processus pathologique et thérapeutique. Cet ordinogramme des
résultats cliniques, des décisions et des alternatives forme un algorithme. |
|||||||||||||||