Annals of the MBC - vol. 2 , n' 4 -
December 1989
MASS BURNS RESCUE
OPERATIONS: ORGANIZATION AND MEDICOSURGICAL THERAPIES
Magliacane G.
Centro Traurnatologico di Torino, Divisione di Chirurgia
Plastica, Centro Grandi Ustioni, Torino, Italia
SUMMARY. A
description is given of general organization in a disaster area, and criteria for triage
of patients are. given. Three homogeneous groups are distinguished on the basis of
expectation of survival: 1) burn patients certain to die with UBS > 100 2) burn
patients with UBS < 100 3) bum patients with lesions < 10-20%. Once the patients
have been subdivided, they follow different routes and therapeutic procedeures, according
to their grouping. In conclusion it is recommended that there should be permanent
communication between the various Burns Centres and between the Centres and decentralized
hospital structures, using information systems with a supporting 2-level infrastructure
integrated by a third nucleus which itself is organized at different levels.
A catastrophe is characterized not only by
the gravity of the event, i.e. the extent of the destruction and the number of victims,
but also by the disproportion between immediate needs and actual means available, which
are never adequate to meet demands. This disproportion is due both to a real shortage of
means and to the difficulty of making full use of them in disaster situations.
It is therefore of paramount importance that all available resources should be properly
employed if full efficiency is to be achieved.
It follows that a good rescue organization is indispensable for optimal performance and a
positive cost / benefit ratio.
These opening remarks, which may seem superfluous, are based on the indisputable
observation made on the basis of a study of the literature that after every disaster
rescue operations have always been conducted in conditions of considerable confusion,
although it should not be forgotten that it is not always easy to act methodically and
rationally in a state of emergency when panic is rife.
The organization of rescue work begins at the site of the disaster and provides for a
whole series of actions, which require for their successful performance a variety of
territorial administrative structures, together with vehicles and means standing by for
this specific purpose.
A large-scale accident with a considerable number of casualties imposes a sanitary
approach with different ethics and deontological principles from those applying in normal
conditions, since the physician has to make himself available for the largest number of
patients possible, using for the less serious patients vehicles and means reserved in
normal circumstances only for the most difficult cases.
This means that certain specialistic structures, normally intended for patients with
little prospects of survival - and therefore employed as a qualitative criterion - must be
reserved to casualties who have a chance of recovery. In this way the highest possible
number of patients may be saved, i.e. the quantitative criterion must prevail.
In these occasions the task of the physician goes beyond mere therapy - he must personally
cope with a variety of organizational problems.
In order to have a better understanding of rescue operations in all their complexity, it
may be useful to outline their main characteristics.
General organization
The site of the disaster can be
subdivided into two main areas: one zone of total destruction, which we will call Zone A,
and, surrounding this, zone B, which can be considered the "operational area".
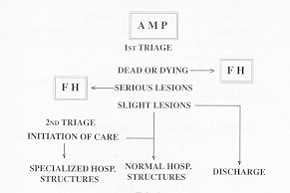
An advanced medication post (AMP) must be set up on the perimeter of Zone B, as near as
possible to Zone A, with the purpose of making a preliminary evaluation of the conditions
of the wounded and to decide upon their immediate destination. Further out, there must be
field hospitals (FH), and depots for medicines, food and material, assembly points for
rescue workers, and emergency quarters for those left homeless by the disaster.
Zone B is thus the operational nerve centre for medical rescue work, which has to be
carried out in Phase 1 by local and possibly non-specialized personnel, and later by
organized structures which must reach the zone as soon as possible.
Zone B is however also the site of the Local Operational Command, which in the initial
phase must coordinate the various rescue activities, make
Group 2: burn patients with UBS < 100 and bum percentage > 18 - 20%;
Group 3: bum patients with lesions < 18-20%.
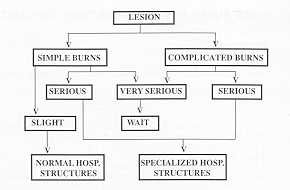
According to their group, patients will follow different therapeutic paths (Tab. 3).
As regards Group 1, if the number of victims is high and the resources limited, in terms
of personnel and means, it may be necessary to make a painful, though inevitable,
selection. Other casualties should not be deprived of necessary assistance, so that Group
1 patients will simply have to be sedated, if possible using a venous route for the
infusion also of hydrating solutions, while being kept apart so that patients in Group 2
can be attended to.
Patients in Group 2 will be immediately sent on to a field hospital, resuscitated and
evacuated with emergency procedures.
Group 3 patients will simply receive medication and be put on a stand-by transfer list,
until Group 2 patients have been evacuated, or until they are dismissed if their burns are
only slight.
In this triage phase it is useful to distinguish the three groups with differentiating
marks (Tab. 4). In this way it is possible to obtain a homogeneous grouping and
consequently a rapid identification of the group required and a further subdivision of the
second group on the basis of therapeutic needs.
 |
Tab. 1 |
| VERY SERIOUS |
USB > 100 |
| SERIOUS |
USB < 100 AND BURN < 18-20% |
| SLIGHT |
BURN < 18-20% |
|
Tab. 2 |
|
Therapy
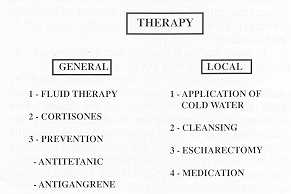
As we have seen, the main therapeutic procedures
concern the second group, which is the group that can best profit from treatment initiated
immediately and correctly carried out. Emergency therapy consists of general and topical
treatment (Tab. 5).
|
Tab. 3 |
LESION |
COLOUR |
MARK |
| VERY SERIOUS |
BLACK |
CROSS |
| SERIOUS |
RED |
HARE |
| SLIGHT |
YELLOW |
TORTOISE |
|
Tab. 4 |
|
Tab. 5 |
| NORMAL
CRITERIA FOR ADMISSION TO A BURNS CENTRE
TOTAL BURNS > 20%
DEEP BURNS > 10%
AIRWAYS BURNS
FUNCTIONAL AREA BURNS |
Tab. 6 |
 |
 |
| Tab. 7 |
Tab. 8 |
| LINK-UP SYSTEMS 1 - "RINW' NETWORK (BCN) between Burn
Centres
2 - "STAR" NETWORK (EN) between Centres and Decentralized structures
3 - OPERATIONAL CENTRE (TN) for transport, linked up with Centres |
Tab. 9 |
|
Fluid therapy must begin as soon as
possible, in order to prevent shock; an indwelling venous catheter must therefore be
inserted, if possible in a central vein, and a bladder catheter. It is advisable to use
simple formulae and only one type of solution, e.g. Parkland's formula (4 ral x % burn x
kg body weight) and Ringer solutions. If these are not available any other type of fluid
containing sodium can be used, bearing in mind that intensive care therapy of the burn
patient requires 0.4-0.6 mEq/kg/bum % of sodium.
Infusion therapy is easier to administer if 3-litre bottles are used, as these do not have
to be changed so frequently. They can be prepared without great difficulty in the field
hospital.
In less serious cases, particularly if the means available are inadequate for the number
of victims, rehydrating therapy can be initiated per os and if necessary continued i.v.
Though not absolutely essential, it is recommended that rudimental laboratory facilities
should be available. In this way it is possible to use micromethods to assess at least the
haematocrit of burn patients who cannot be immediately transported to hospital.
It is advisable in all cases to monitor hourly diuresis.
Pharmacological treatment must be reduced, being limited to the use of cortisone
preparations in cases of shock, sedatives and analgesics, as necessary.
Antibiotic therapy is counterindicated at this stage. This form of therapy is always
reserved for later stages of the burn illness, in cases when sepsis is demonstrated and
when a biogram has been performed.
Antitetanus and if necessary antigangrene therapy should be performed.
Mild antiseptics, e.g. chlorhexidine, must be used topically for summary cleansing, after
careful removal of clothing, followed by the application of occlusive dressings with
antibacterial agents, e.g. silver sulphadiazine.
In hand burns, the use is recommended of lisle gloves impregnated with silver
sulphadiazine.
In caustic bums, the part afTected must be thoroughly washed in order to dilute the
chemical agent and prevent deepening of the lesion. This phenomenon occurs not so much
because of the thermal effect as of the chemical reaction between the caustic agent and
the skin, due to oxidation, reduction and formation of salts, with protein coagulation;
this continues until the reaction caused by the chemical agent is completely exhausted.
If the patient has been exposed to radiation, he must be isolated, subjected immediately
to external decontamination by washing and prolonged showers and complete depilation; the
lesions must be amply and radically cleansed, and then dressed. In cases of
circumferential bums, releasing escharectomy must be performed in order to keep the
circulation free in the limbs, or to allow normal breathing when the thorax is
incarcerated.
If immediate transfer is expected it may be sufficient to wrap the patient in lengths of
cloth or disposable sterile material, protecting the patient from heat loss which
negatively atTects later metabolic imbalances.
Treatment on the spot necessarily has considerable limitations: the shortage of time
available for each casualty and the impossibility of predicting when and how the patient
will be transferred do not create ideal conditions for treatment, as the physician can
never be sure of completing even the simplest of therapeutic protocols.
Another problem is that after the first 48-72 hours metabolic complications begin to
appear, together with infective complications, and these cannot be treated at the disaster
site.
At this point the patients have to be transferred to suitable hospital facilities. A
further triage has to be carried out to distinguish between patients needing treatment in
a Burns Centre and those who can be sent to a less specialized structure.
Let us recall the fundamental conditions that impose admission to a Bums Centre (Tab. 6):
- T13SA > 20%
- full-thickness burned area > 10%
- presence of burns in functionally important areas, such as
the face, hands, perineum and joints
- electrocution
- bums to the airways
- bums complicated by associated traumas or concomitant
and/or pre-existing diseases.
In the event of a catastrophe, the use of
hospital facilities will necessarily be determined by the relationship between the number
of beds available and the number of patients needing admission.
If the number of casualties is high, it is advisable to create - in those hospitals which
already possess a specialized Centre, or where there is a specialized medical team capable
of handling bum victims -facilities that transform routine therapy wards into wards
equipped for the treatment of bum victims, so that the number of casualties that can be
admitted is considerably increased.
If the bum lesion is not particularly serious, and especially if accompanied by other
traumas, the patient can be admitted to any large general hospital where he can be treated
with specialist care.
If the lesions are of small account, but still require treatment, the patient can be
admitted to small local hospitals.
Problems arise when there are not enough hospital beds for all the patients who could
benefit from admission to a specialized Centre or from treatment given by bum specialists.
Although we are aware that in actual practice any theoretical suggestions have little
chance of being followed, we would like to put forward some points that may be of some
assistance to the physician on the spot when he has to proceed to the dispatch of patients
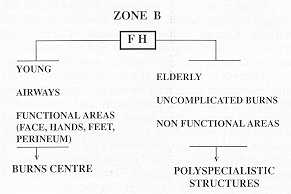
to appropriate destinations, in relation to the clinical situation (Tab. 7).
Young patients and those with suspected damage to the airways, or with burns in the
anatomical sites mentioned above which are important for functional recovery, should be
transferred to Burn Centres, where they will receive the treatment they need.
The method of transfer and in particular the choice of vehicle depends on the distance
from the site of the accident and the final destination -ambulances or buses may be
sufficient for short journeys and aeroplanes for longer distance.
Conclusions
The scientific literature and the
daily newspapers report numerous episodes of mass bums caused by natural disasters
(earthquakes or forest fires), military incidents (apart from the battlefield), such as
the explosion of ammunition dumps or acts of terrorism, and urban accidents of industrial
origin or due to means of transport.
The first priority is that every nation should identify the zones, situations and the type
of potential risk, so that rescue resources can be made immediately available and proper
preparations can be made for keeping the disaster under control.
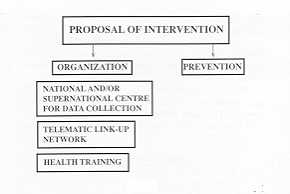
It is advisable to approach the problem from two directions, i.e. that of prevention and
that of organization (Tab. 8).
The question of prevention is so complex that it needs to be treated separately.
With regard to organization it is possible to identify some fundamental points, which have
to be constantly reviewed in order to improve on the results of previous experiences.
The first absolute priority is the creation of a national and supernational body that will
centralize all information regarding the various types of disaster, with particular
reference to medical data, such as the number of dead, the type of lesions, the measures
undertaken, the results obtained and the deficiencies observed.
This would make it possible to create work groups capable of coordinating all the data
collected and of making opportune proposals.
The medical and paramedical stafT operating in health facilities in the risk zones must
learn the essential elements of burn pathology by attending refresher courses and
attending specialized units. In this way it will be possible to achieve standardization of
materials and methods.
It is also very important to create permanent communications between the various Burns
Centres in the territory and between the Burns Centres and decentralized hospital
structures. This can be done by means of distributed information systems, creating a
supporting infrastructure at two distinct levels and completed by a third nucleus, which
in turn is itself organized at different levels.
This purpose could be achieved by computer networks which, working together, could link up
a number of widely distributed computers and organisms.
The structure of the system could include (Tab. 9):
- a nationwide, interactive "ring" network
connecting all specialized Centres, organized with several interacting computers (Burns
Centre Network BCN);
- A regional or multiregional "star" network, at a
lower hierarchical level, linking up General Hospitals with the nearest Burns
Centre, and enabling various organisms to link up with this Centre, interacting by
computer in emergency situations in order to arrange admission to sanitary structures
other than the Centre but dependent upon it (Emergency Network = EN);
- an operational Centre responsible for nationwide patient
transfer, linked up with the "ring" network (Transfer Network) = TN). The BCN
will have to guarantee information flow, including the availability in real time of
beds in the various national Centres.
The EN would permit the use of
non-specialized units for the admission of burn patients under the diagnostic and
therapeutic care of the principal Centre in the network.
In other words, in the event of mass burns, the ring" network would make it possible
to fill all national Centres without any waste of time, after which the "star"
network would make it possible to use the General Hospitals nearest to the disaster area.
The task of the TN is the organization of vehicles and operational details for providing
transport. Thus, through its link-ups, it must locate and mobilize the necessary means of
transport, prepare flight plans and/or other methods of transport necessary for the
mission, and give advance warning to services in the place of destination so that land
transport facilities are coordinated. This network can make use of pre-existing services
in other organized structures, such as the Army, the Police, the Fire Brigade and the Red
Cross. These organizations must however coordinate their activities, finalizing them to
the same objective and linking up with the Burns Centres.
RESUME. L'Auteur, après avoir
traité l'organisation générale dans la zone du désastre, considère les paramètres
pour le triage des patients, qui sont divisés en trois groupes homogènes sur la base de
leurs possibilités de survie: Groupe 1: brûlés avec pronostic sûrement funeste; Groupe
2: brûlés avec UBS < 100; Groupe 3: brûlés avec lésions < 10-20%. Une fois
divisés, les patients suivent des percours et des procédés thérapeutiques différents,
selon le groupe d'appartenance. Enfin l'Auteur propose la création d'un dialogue
permanent entre les divers Centres des Brûlés et entre ceux-ci et les structures
hospitalières périphériques, en utilisant les systèmes d'informatique avec une
infrastructure de support à deux niveaux complétée par un troisième noyau à son tour
organisé à divers niveaux.
|