Annals of the MBC - vol. 2 - n' 4 -
December 1989
HEALTH CARE IN
DISASTERS - GENERAL CONSIDERATIONS
Quetglas J.
Madrid, Spain
SUMMARY. The
Los Alfaques fire disaster, in which 102 people were killed and 148 sustained burn
injuries when a tank containing propylene exploded near a holiday camp, prompted a
revision of the plans for care in the event of a bums catastrophe. Two alternative plans
are, described, one for war-time, one for peace-time. A proposal is made that the
Mediterranean Bums Club should establish a Commission of Health Care in Fire Catastrophes
that would have the task of advising countries or organizations requesting information.
In the recent history of Europe we find
numerous cases of catastrophes caused by fire as the consequence of industrialization and
of accidents.
History therefore shows us the constant need to be prepared to face such disasters. It is
universally true that unfortunately there were many dead and few wounded in these
accidents, with the exception of Los Alfaques. It is undeniably true that nothing can
justify carelessness in the foresight and preparation of health care in such
circumstances.
1 believe this is one more task of the Mediterranean Burns Club in the nations washed by
Mare Nostrum.
Not wishing to go into details regarding other nations, 1 would like to consider one of
the greatest fire disasters in Spain, the Los Alfaques disaster, where a traffic accident
led to the explosion of a tank containing propylene, setting fire to a holiday camp on the
Mediterranean beach. An area of over 10,000 square metres was affected. There were 102
deaths and 148 burn casualties, of whom 122 had over 50% burned surface area.
For the evacuation of the burned patients two routes were established, one towards the
north, Barcelona, where 58 patients were sent, and the other towards the south, Valencia,
where 82 patients were sent. The rest were evacuated directly to their home countries -
there were many foreign tourists in the camp.
An average of 24% of the burn patients sent both to the north and the south had 80% or
more BSA.
The health care in the burn centres in both destinations was similar and first-class, but
the health care during evacuation was totally different.
Survival rate after four days was 93% for the north route and 45% for the south.
Afterwards we observed that the survival curve descended progressively in the north while
it was flat in the south, so that after two months the curves were equal. We believe it
would be interesting to analyse this effect, but it goes beyond the scope of this paper.
At the time of the disaster 1 held the post of Chief of Plastic Surgery Service at the
Central Military Hospital and 1 carried out a revision of the plans of care in
catastrophes. We established two possibilities: one for health care for burned patients in
wartime, and another for health care in civil catastrophes in peacetime.
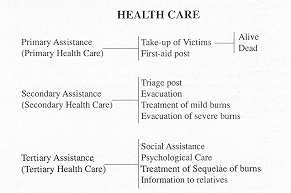
Clearly the situations are totally different, although the same idea prevails in both -
rapid evacuation in the best possible conditions towards specialized Burn Centres for
treatment.
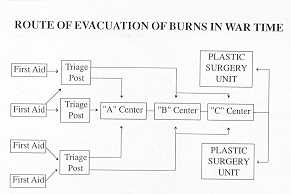
In wartime the evacuation route would be established in the following way: from first-aid
post to triage centre and from here to an advanced or intermediate Burns Centre or to a
rearguard Burns Centre and ultimately to a Plastic Surgery Unit.
In brief, our plan consists essentially in establishing intermediate Burns Centres in the
line of evacuation to assure continuous and efficient care. Each of these centres would
have specific missions and structures. Thus the "A" centre would be placed very
near the combat zone; its function would be triage and resuscitation, not treatment or
hospitalization. The "B" centre would have a function of revision of treatment
and preparation of the patients for further evacuation. This centre would treat moderate
and mild burned patients who would soon recover, and also care for shock, changin bandages
and preparation of severe patients for evacuation. The "B" centre does not have
a definitive treatment task. The "C" centres would have a function of integral,
general and local treatment of all patients, except that of burns sequelae which would be
treated in the Plastic Surgery Unit.
We consider as fundamental the task of the triage post, where the staff must be very well
prepared and trained. They need not necessarily be physicians but they must be well
acquainted with bum pathology so that they can orient efficiently the direction and
destination of each burned patient, and institute treatment.
With regard to health care in civil catastrophes in peacetime we planned a system of total
care based on our ideas and knowledge of the problem.
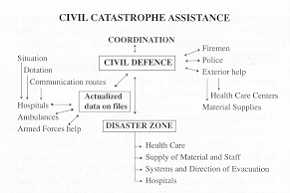
The first essential condition is perfect coordination between all rescue posts. A single
Command is therefore necessary, which in this case would correspond to the Civil Defence
Authority or its Delegate. This coordination should be maintained not only for health care
but also for the supply of materials, personnel, coordination with the Police and Fire
Service, data regarding bed availability in hospitals, etc.
The catastrophe zone must be divided into sub-zones according to the degree of
destruction. In general terms we consider three sub-zones: that of first aid, of rescue,
and of support.
Sub-zone 1 health care is limited to collecting the victims and evacuating them. Sub-zone
2 is the site of triage centres, which is the most important function in these cases; it
also establishes evacuation routes. Sub-zone 3 health care centres are set up for burn
patients with mild or severe injuries who will need treatment. In special cases very
severe burn patients would be evacuated to more specialized centres.
This support sub-zone has the task of storing and supplying the necessary means and also
of selecting the sanitary centres that would receive the burns patients for definitive
treatment or for referral to other centres, once they have been adequately prepared for
evacuation.
1 would like to recall that the evacuation of burn patients must be performed with certain
minimal guarantees and as quickly and comfortably as possible, in conditions that will
ensure continuous care during transportation and avoidance of bum contamination.
 |
Area 1. Of greatest
destruction. Requires all exterior help. Primary Health Care: Collection and evacuation of
victims. |
|
Therefore it is necessary to reserve
medicalized ambulances for severe cases and to use unmedicalized ambulances for those
cases of mild or moderate injuries which do not require treatment during transport.
Transportation will be performed by a variety of means, stretchers, ambulances, etc. Air
transportation is the best means, either by ordinary aeroplanes or by helicopter. However
it must be taken into account that these machines have a relatively short range, even
though it is now increasing. The helicopter has a range of between 200-400 miles,
depending on the possibility of refuelling when reaching the centre. Another handicap is
their dependence on weather conditions, and in the case of aeroplanes, there is the need
of an airport.
Transportation by helicopter is considered almost ideal because in spite of the drawbacks
(noise, lack of pressurization, etc.) the helicopter, besides its speed, has the
possibility of providing adequate treatment during evacuation.
1 would like to dedicate here a word of homage to the great French surgeon Larrey, who was
the first to use air evacuation during the Franco-Prussian war, evacuating 160 patients
with aerostatic balloons during the siege of Paris.
 |
Area 2. Damaged but
usable. Needs exterior help. Primary and Secondary Health Care: Triage Centres. Treatment
of mild bums. Evacuation. |
|
And with special reference to burns 1
would like to recall another French surgeon Chaisagne, who in 1915 had already observed
that the burns of aviators evolved better than trench bums and attributed this also to the
rapidity with which the aviators reached hospital.
Railroad evacuation should not be forgotten. In certain cases it offers the great
advantage of making a real hospital available with the possibility of surgical procedures.
All this is easy to design on paper and beautiful to show in slides, but it is difficult
to put into practice when the catastrophe unexpectedly arrives.
Therefore 1 would like to make a proposal to the Executive Commitee of the Mediterranean
Burns Club: to establish a Commission of Health Care in Fire Catastrophes, similar to that
which exists in Scandinavia with KAMEDO, but with a larger projection and greater
responsibility.
This Committee would have the task of advising countries or organizations about plans for
health care in catastrophes.
|
Area 3. Undamaged.
Will send help. Secondary and Definitive Health Care: Burns Centres. Evacuation of very
special cases. |
|
It would advise and help in the training
of health personnel, and make available adequate equipment for direct help with material
and staff when a catastrophe occurs, when requested by the authorities of the nation
affected; it would also be in a position to put at its disposal Burns Centres where
patients could be treated. These Centres would have previously agreed to receive foreign
patients for treatment.
In this manner the Mediterranean Bums Club will be able to contribute efficiently to the
creation of an organization of specialized professionals who will study the problem of the
prevention and care of bums catastrophes in all the Mediterranean countries. Every country
will prepare plans which should be continuously up-dated and which would be put into
operation disinterestedly with any nation needing not only consultants but also the
despatch of personnel and materials, in order to face the difficult task of care, rescue
and rehabilitation in the disaster zone.
This proposal is perhaps very ambitious but we believe it comes within the scope of our
Mediterranean Bums Club. This task could be the expression of a high and altruistic ideal
for the nations washed by our Mare Nostrum.
RESUME. L'incendie désastreux de
Los Alfaques, quand 102 personnes sont mortes et 148 ont subi des brûlures à la suite de
l'explosion d'une cisterne de propylène, a provoqué, une révision des plans pour les
soins en cas d'un incendie catastrophique. Deux alternatives sont décrites, l'une pour
une periode de guerre, l'autre pour une période de paix. L'Auteur avance la proposition
que le Club Méditerranéen des Brûlures crée une Commission de Soins Sanitaires en cas
de d'hucendie Catastrophique, qui devrait conseiller les pays et les organisations qui
demandent des informations.
BIBLIOGRAPHY
- Arturson G., Blomberg R.: El desastre de los
alfaques. Cir. Plast. Iber Latinamer., 6: 163, 1980.
|