| Annals of the MBC - vol. 3 - n' 1 - March 1990
SURGICAL TREATMENT OF POST-BURN CONTRACTURES OF THE HAND
Caleffi E., Bocchi A., Toschi S., Ghillani M.
Divisione di Chirurgia Plastica, Parma, Italia
SUMMARY. When static and
dynamic splints fail to improve the functional and aesthetic outcome of post-burn
contractures of the hand, surgery is often found to be necessary. The only surgical
procedure that offers satisfactory results is the flap technique. Three case histories are
described.
In post-bum contractures of the hand
surgical treatment is often necessary when prevention by means of splints has failed to
improve the functional or aesthetic outcome. According to Tajinia (1), corrective splints
can be classified in two types: static and dynamic.
The former exert a self-controlled corrective force on joint stitTness; dynamic splints
exert a constant corrective force by the elasticity of a rubber band or wire spring.
Improvement with corrective splinting is usually remarkable in the first two weeks and
then gradually slows down in a month or two. However, splintage should be continued until
there is no further improvement (2, 3). In our experience there are several major types of
post-bum contracture involving the volar and dorsal side of the hand: flexion contracture
of the MP joint, flexion contracture of the PIP joint, adduction contracture of the thumb,
and extension dorsal contracture. A surgical scar excision may also be necessary for
oncologic reasons: a squamous carcinoma may arise on a bum scar. Debridement of scar
tissue and correction of joint (4) contracture must be followed by flap coverage: in our
experience the use of a skin graft to replace the scarred skin has often caused recurrence
of the contracture and failure of the surgical treatment.
Various types of flap can be used to resurface the hand after debridement: in our series
we have more often used an island radial sensitive flap or an abdominal or brachial flap.
We report a few cases to illustrate our technique and surgical refinements.
Case report 1
A 30-year-old woman sustained a bum of the left hand Aich
caused severe flexion scar contractures of the MP and PIP joint of the third and fourth
finger (Fig. 1).
 |
Fig. 1 a) Pre-operative
view: impressive flexion contracture of 3rd and 4th finger |
 |
Fig. 1 b) Intra-operative
view |
 |
Fig. 1 c)
Final result at 1 year |
|
Her thumb was also involved by the bum and
a hypertrophic scar was present.
First we performed a complete debridement of the scar tissue and correction of the NIP and
PIP flexion by the use of Kirschner wires. The coverage of the volar defect was obtained
with a cross-arm flap. The patient refused correction of the thumb scar.
Three weeks later we completed the reconstruction: the patient began rehabilitation and at
10 months both functional and cosmetic results were satisfactory.
Case report 2
A 22-year-old man sustained bums of the
face, arms, hands and lower extremities. All bum areas were resurfaced with
split-thickness skin graft (Fig. 2).
 |
 |
| Fig. 2 a)
Pre-operative view: adduction contracture of the thumb |
Fig. 2 b) Final
result after correction of the right hand with an abdominal flap |
|
A severe contracture of the first web of
both hands was the result of the bum healing and scarring of grafted skin. The contracture
imposed a surgical procedure initially at the level of the right hand. the first web was
reconstructed by means of an abdominal flap. At 9 months the functional improvement was
impressive and the cosmetic effect was also satisfactory.
The patient did not return for treatment of the left hand.
Case report 3
A 45-year-old man sustained a bum of the
volar side of the hand. A contracture of the first web and chronic ulceration of the bum
scar developed during the following months. Debridement of the scar tissue was performed;
an island sensitive radial flap was carried out to reconstruct the first web and thenar
region. 8 months after the operation the functional and morphological results were
excellent, with recovery of sensitivity (Fig. 3).
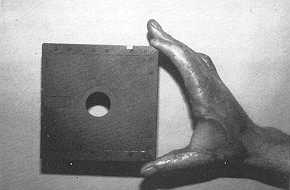 |
Fig. 3 a)
Pre-operative view: chronic ulceration of a burn scar with developing contracture of the
first web |
 |
Fig. 3 b)
Intra-operative view: the island radial flap |
 |
 |
| Fig.
3 c)-d) Post-operative view 8 months later |
|
Discussion
Post-bum contractures of the hand require appropriate
surgical treatment whenever conservative approaches have failed.
The purpose of every surgical operation is to carry out a stable coverage of the involved
area and to avoid recurrence of contracture or chronic ulcers or breakdown. In our series
satisfactory results have been obtained using forearm radial flaps or abdominal or
brachial flaps transferred to the hand by means of cross-arm. flaps.
A radial forearm island flap can be used in a single intervention to release severe
contractures of the first web, thenar region, and dorsal region using its complete
rotation arc. We can also restore sensitivity to the Injured hand. The cross-arm flaps
(abdominal or brachial) do not restore sensitivity and impose on the patient considerable
immobilization; also, the use of skin grafts is not effective to improve the functional
aspect and to ensure a stable result; the recurrence of contracture or chronic breakdown
is often observed and a second surgical operation is necessary.
Therefore the use of a flap is the only surgical procedure that ofrers functionally and
cosmetically satisfactory results.
RÉSUMÉ. Quand les appareils statiques
et dynamiques ne sont pas suffisants pour améliorer le résultat fonctionnel et
esthétique des contractures à la suite des brûlures, il faut souvent recourir au
chirurgien. La technique du lambeau est la seule procédure chirurgicale qui offre des
résultats positifs. Les Auteurs présentent trois cas.
BIBLIOGRAPHY
- Tajima E: Treatment of post-traumatic contracture of
the hand. J. Hand Surg., 13: 118-129, 1988.
- lbaraki K., Tajima T., Watanabe Y., Seki T.:
Analysis of the effect of corrective splinting and operative release in the post traumatic
contracture of finger joints.
- Kraemer M.: Burns contractures: incidence,
predisposing factors and results of surgical therapy. J. Bum Care, 9: 261-265, 1983.
- Cannon B., May LW: Skin contractures of the hand.
In: J.E. Flynn (ed.), "Hand Surgery", 3rd ed., Williams and Wilkins, Baltimore,
776-785, 1982.
|