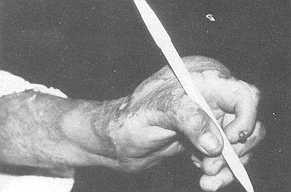
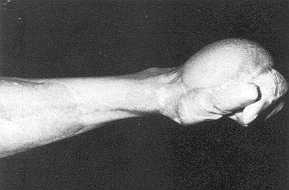
Annals of the MBC - vol. 3 - n' 1 - March 1990 METACARPO-PHALANGEAL JOINT RELEASE IN THE MANAGEMENT OF POST-BURN STIFF HANDTarek Atta A., Rizk A., Ismail M. Departments of Plastic Surgery and Orthopaedics, Faculty of Medicine, Cairo University, Egypt SUMMARY. The present work presents the use of metacarpophalangeal (M.P.) joint release in the management of 20 cases with post-bum stiff hand. The paper presents a new modification of the technique of M.P. capsulectomy. The principle of our method of treatment is that we release the origin of the collateral ligaments, dorsal capsule and the deep transverse metacarpal ligament from the metacarpal head from within the joint through a dorsal incision in the capsule. After closure of that incision, the joint is left with an intact soft tissue sleeve around it, formed by the periosteum of the metacarpal, the joint capsule and periosteum of the proximal phalanx. This soft tissue sleeve will stretch enough to allow the joint to be flexed and the metacarpal arch to be regained. This position is maintained by Kirschner wires transfixing the joint, so that the ligaments and the dorsal capsule will get a more distal attachment to the metacarpal heads. Thus, the stability of the joint is not jeopardised. In the meantime, the dorsal contracted skin is replaced with healthy suitable skin cover. In conclusion, M.P. joint release in the management of post-bum stiff hand is recommended, as evidenced by the good post-operative hand function in the cases described. Introduction Immobility of the metacarpophalangeal (M.P.) joints and post-burn swelling with the deposit of oedema fluid about the ligamentous tissues and the extensor tendons lead to adhesions of the extensor mechanism, to contracture and adhesions of the collateral ligaments, or to thickening of the entire capsular ligamentous structure. Post-burn scar contracture adds more stiffness and disability to the injured hand (2). Split skin graft after scar release and excision is the traditional line of treatment. This is aided by putting the hand on a slab or applying gradual post-operative traction over the stiff joints to stretch the contracted ligamentous structures (6). As the pathology is fibrosis, adhesions and contracture, capsulectomy of the M.P. joints associated with scar excision is considered in the management of neglected post-burn stiff hands (1, 3, 7). Material and methods The present work included 20 patients suffering from post-burn contracted scar of the dorsum of the hand. In all the cases there was stiffness of the M.P. joints. The extra-articular ankylosis of the M.P. joints was diagnosed on both clinical and radiological bases. The time since the burn ranged from one to six years. Metacarpophalangeal joint release and capsulectomy after scar excision and release were performed in all the cases. In four cases the procedure was carried out for the M.P. joint of the thumb and in 16 cases for the M.P. joints of the medial four fingers. Operative Procedures Under general anaesthesia and tourniquet, scar excision and release of the dorsum of the hand are performed down to the paratenon of the long extensors of the fingers. The extensor hood and the long extensor tendons are split longitudinally for 2 cm on either side of the M.P. joint. The aponeurotic or extensor hood is retracted to either side. The dorsal capsule is opened by a longitudinal cut that extends over the periosteum of the metacarpal bone and the proximal phalanx for 1 cm (Fig. 1). From within the capsule of the M.P. joint, we release the attachments of the collateral ligaments on both sides of the joint, the deep transverse metacarpal ligament from the metacarpal head and the dorsal capsule together with elevation of the periosteum of the metacarpal bone and the proximal phalanx for about 1 cm on both sides of the M.P. joint (Fig. 2). At this stage the head of the metacarpal bone and the base of the proximal phalanx should be freely mobile.
The dorsal incision of the capsule can now be closed with interrupted simple 4/0 Dexon stitches. The joint is now covered by intact soft tissue sleeve formed by the periosteurn of the metacarpal bone, the joint capsule and the periosteum of the proximal phalanx. This soft tissue sleeve will stretch enough to allow the M.P. joint to be fixed to 90' and the metacarpal arch to be regained. This position is maintained by Kirschner wires transfixing the joint. The split extensor hood and extensor tendons are then sutured by interrupted simple 4/0 Dexon stitches. Covering of Resultant Skin Defect
Results The oedema fluid following the burn hydraulically drives the M.P. joint into extension. This position increases flexor tension and decreases extensor tension, so the fingers are flexed at the interphalangeal joints and hyperextended at the M.P. joints. When the hand is neglected in this position contracture develops. Moreover contracture of the burned skin on the dorsum of the hand will maintain and increase the deformity. The contracture around the M.P. joint is mainly an adaptive thickening of the deep transverse metacarpal ligament, dorsal capsule and collateral ligaments (7). The shortening of the collateral ligaments will prevent flexion of the M.P. joint because of the cam effect of the metacarpal head. Also, shortening of the deep transverse metacarpal ligament will obliterate the normal palmar concavity, which leads to marked weakening of the grip.
Buch (1) and Curtis (2) described
capsulectorny of the M.P. joints in cases of the rheumatoid hand and recommended its use
in cases of post-burn stiff hand. The technique as described by Curtis (2) entails
excision of a transverse wedge of the dorsal capsule of the M.P. joint; the cordlike
portion of the collateral ligaments are then severed near their metacarpal attachment on
both sides leaving the accessory collateral ligaments to stabilise the joint.
RÉSUMÉ. Les Auteurs décrivent l'emploi du relâchement des articulations métacarpophalangiennes (M.P.) dans le traitement de 20 patients avec la main rigide à cause de brûlure. Ils présentent une nouvelle modification de la technique de la capsulectomie M.P. Cette méthode est recommandée puisqu'elle permet le recouvrement d'une bonne fonction de la main. BIBLIOGRAPHY
|