Annals of the MBC - vol. 3 - n' 1 -
March 1990
POST-BURN
CONTRACTURE OF THE AXILLA EVALUATION OF THREE METHODS OF MANAGEMENT
Higazi M., Mandour S., Shalaby H.A.
Plastic Reconstructure Surgical Unit,
Faculty of Medicine, Tanta University, Tanta, Egypt
SUMMARY.
The surgical correction of 32 post-burn contractures of the axilla was evaluated using
skin graft, Z-plasties and scapular flaps.
Introduction
The goal of the surgical correction of
axillary scar contractures is to provide a maximum release with minimum or no local
anatomic distortion. Once surgical correction is intended, the choice of the procedure
must be individualized. Traditional therapeutic measures include skin grafting, Z-plasties
and local flaps, but these methods do not always produce satisfactory results. More
recently such methods as the free flap (1) and the island flap (2,3) have been reported.
In these newer methods, a flap of sufficient thickness with less likelihood of recurrence
and no need for splinting is inset into the axilla.
In this paper, we report the correction of 32 axillae in 30 patients (17 male and 13
female) by split skin graft, Z-plasties and scapular flaps.
Material and methods
Based on the local anatomic conditions
of the axilla, the surgical procedure was selected. Hanumadass et al. (4) classified
axillary contractures in 4 types depending on three local anatomic conditions:
- - Anterior and posterior axillary folds
- - Hairbearing area
- - Scarring of adjacent skin.
Our patients were classified in three
groups according to the line of management.
Group 1 12 axillae (Types 11, 111 &
IV) were treated by release and split skin graft (S.S.G.):
(a) 7 axillae by single release and graft
(b) 5 axillae by double release leaving a central bridge of normal or scarred tissue at
the apex of the axilla (Fig. 1) as recommended by Salisbury and Pruitt (5).

|
Fig. 1: Double
release, central skin bridge and SSG of upper and lower raw areas. |
|
Group II 14 axillae (Type 1) were treated
by Z-plasties:
(a) Single Z-plasty (5 axillae)
(b) YN advancement (3 axillae)
(c) Double Z-plasty with YN advancement (Five-flap technique) (6 axillae).
In the latter technique (Fig. 2) the CDE
flap enclosing the hair-bearing area is minimally advanced and undermining was carried out
on the undersurface of the web.
Group III 6 axillae (Types II, III & IV) were treated by scapular flaps.
The circumflex scapular artery passes through the triangular space and then courses around
the lateral border of the scapula and directs itself toward the cutaneous territory of the
back. There are two cutaneous branches, the horizontal (scapular) and oblique
(parascapular). A flap that has the circumflex scapular artery as its nutrient vessel can
therefore be designed in one of two directions: the scapular and the parascapular (6).
The pedicle is located by drawing a line (with the arm fully adducted) from the top of the
posterior axillary fold to the lateral border of the scapula. Just adiacent to this border
lies the triangular space and the vascular pedicle. In scarred and distorted anatomy of
the posterior axillary fold the dissection is started from medial to lateral before
locating the,pedicle. The donor area was closed primarily in a11 of our cases (6-10 cm
breadth).
|
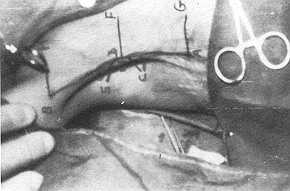
Fig. 2: Five flap
technique, the triangle carrying the hair bearing area is minimally advanced. |
|
Results
Thirty patients having 32 post-burn
contractures of the axillae were included in this'study, 15 cases (506/o) in the age group
1-10 years (Table 1). The cause of bum is illustrated in Table 11. It shows that 63% were
scalds. Table 111 shows the degree of contracture and Table IV the anatomical site of
contracture.
The results were evaluated according to the criteria of Davies and Yacournattis (7):
- Good: when full mobility with lax skin was found at the
time of evaluation
- Fair: when local discomfort or tight skin impaired full
mobility but did not require secondary operation
- Bad: impaired function requiring secondary operation.
Age group |
No of cases |
% |
| 1 - 10 years |
15 |
50.00 |
| 11-20 years |
5 |
16.70 |
| 21-30 years |
8 |
26.70 |
| 31-40 years |
1 |
3.30 |
| 41-50 years |
1 |
3.30 |
| Total |
30 |
100 |
|
Table 1 AGE OF
PATIENTS |
|
Type |
No
of cases |
% |
Scalds |
19 |
63.30 |
Flame burn |
11 |
36.70 |
Chemicals |
0 |
0 |
Electric |
0 |
0 |
Total |
30 |
100 |
|
Table II CAUSE OF
BURN |
|
| Degree of abduction at the axilla |
No |
% |
| Mild contracture (above 90') |
6 |
18.75 |
| Moderate contracture (30-90') |
20 |
62.50 |
| Severe contracture (below 30') |
6 |
18.75 |
| Total |
32 |
100 |
|
Table III DEGREE OF
CONTRACTURE IN 32 CONTRACTED AXILLAE |
|

|
Fig. 3: SSG
on a single release, one year postoperative. Note recontracture of the anterior axillary
fold. |
|

|
Fig. 4: Double
release and SSG, 9 months postoperative. |
|

|
Fig. 5: Double
release and SSG, loss of the graft on the lower area. Regrafting was followed by
satisfactory result. |
|

|
Fig. 6:
Five flap technique, 9 months postoperative. |
|
The follow-up of our cases ranged from 6
months to 1.5 years with a mean of 11 months.
- Single incision and SSG (Fig. 3):
- 7 cases treated by this method
- 2 cases partial graft loss and regrafting
- 2 cases evaluated good, 3 fair and 2 bad result
- Hyperpigmentation of the grafted areas manifest in 3 cases
- Double incision and SSG:
- 5 cases treated by this method
- 4 cases evaluated good at their last follow-up (Fig. 4). *
I case (Fig. 5) lost the graft on the lower area that was regrafted with final fair result
at evaluation * Hyperpigmentation of the grafted area manifest in 4 cases
- Single Z-plasty:
- This method used in 5 cases
- Final result at evaluation good in 3, fair in 1 and bad in
1 * The displacement of the hair-bearing area was manifest in the 4 successful cases
- YN advancement flap:
- 3 cases treated by this method Evaluated as good in all
Displacement of the hair-bearing area was also evident in all cases
- Five-flap technique:
- 6 cases corrected by this method All evaluated good (Fig.
6) Displacement of the hair-bearing area was minimal
- Scapular flap:
- 6 cases corrected by this method All evaluated good,
functionally a good

|
Fig. 7: a)
Scapular flap, immediate postop. |
|

|
Fig. 8: Widening
of the donor area with maceration of the edges. One week postop. |
|
Discussion
The feasibility of a particular
procedure depends on a set of particular local anatomic conditions. The main' problem of
axillary contractures is the inelasticity of either or both axillary folds which prevents
the full extension and/or abduction of the shoulder joint. There are two local anatomic
conditions that must be taken into consideration when surgical correction is intended. These
are the amount of scarring of the folds and adjacent skin, and the involvement of the
hair-bearing area.
In this study split skin graft was satisfactory when applied on a double release incision.
The central flap created by the incisions or by mobilization of anterior and posterior
bridges aids in preserving the hair-bearing area and the successful take of the graft.
This also minimizes the tendency of the grafted axilla to recontract. This tendency of
split skin grafted area was reported by many authors (8, 9, 10), and continuous splinting
and massage for 3-6 months were suggested.
Z-plasty is generally the procedure of choice for linear scar contractures. However, a
single Z-plasty is not suitable in the axillary contracture, because it requires large
skin flaps in a limited area with displacement of the hair-bearing area. We found that
five-flap Z-plasty is more suitable for this type of contracture. The hair-bearing area
was displaced to a lesser extent in this technique. This finding coincides with that
reported by other researchers (11, 12).
The cutaneous blood supply of the scapular region was described by Salmon (13). Dos Santos
(14, 15) demonstrated the clinical application of the scapular flap. Mayou et al., (16)
and Diamond and Barwick (2) each reported one case.
The scapular flap was successful in our six cases. It is a versatile flap combining a thin
cover in most cases with direct closure of the donor defect. It was used in a
superficially scarred scapular area as it is a fasciocutaneous flap including a known
artery as its pedicle.
Free flaps (1) have been used but they are technically more difficult, require longer
anaesthetic time and a trained microvascular surgeon. Also, latismus dorsi or pectoralis
major myocutaneous flaps have been used (17), but the extra bulk of the muscle would
appear to limit the adduction of the shoulder.
Conclusion
- - For axillary web contractures the five-flap technique is
the procedure of choice.
- - Scar contracture of the anterior and/or posterior
axillary folds with scarring of adjacent skin, but sparing the hair-bearing area, is
preferably corrected by double incisional release and split skin graft.
- - In scars involving the hair-bearing area usually with one
or both axillary folds as well as the periaxillary skin, i.e. a diffuse car contradture,
the procedure of choice is the scapular flap. The parascapular flap is another alternative
which is being evaluated in our unit.
RÉSUMÉ. Les Auteurs
considèrent 32 cas de correction chirurgicale des contractures de l'aisselle, à la suite
de brûlure, avec l'emploi des greffes cutanées à épaisseur variable, des plasties en Z
et des lambeaux scapulaires.
BIBLIOGRAPHY
- Ohmori S.: Correction of burn deformities using free
flap transfer. J. Trauma, 22: 104, 1982.
- Diamond M., Barwick W.: Treatment of axillary burn
scar contracture using an arterialized scapular island flap. Plast. Reconstr. Surg., 72:
388, 1983.
- Budo J., Finucan T., Clarke J.: The inner arm
fasciocutaneous flap, Plast. Reconstr. Surg., 73: 629, 1984.
- Hanumadass M., Kagan R., Matsuda T., Joyaram B.:
Classification and surgical correction of postburn axillary contractures. J. Trauma., 26:
236, 1986.
- Salisbury R.E., Pruitt B.A.: Burns of the upper
extremity. In Pruitt B.A. (ed): "Major Problems in Clinical Surgery", 19, 154,
Saunders, Philadelphia, 1976.
- Takato T., Harii K., Sasaki A,: Our clinical
experience with the scapular flap. Jpn. J. Plast. Reconstr. Surg., 27: 318, 1984. Cited
from Yanai et al., Plast. Reconstr. Surg., 76: 126, 1985.
- Davies D.M., Yacournattis A.M.: A method of grafting
hand burns following early excision. Br. J. Surg., 65: 539, 1978.
- Rintala A.E., Pironen J.: Secondary reconstructive
surgery in burns. Ann. Chir. Gynecol., 69: 233, 1980.
- Tolhourst D., Haeseker B.: Fasciocutaneous flaps in
the axillary region. Br. J. Plast. Surg., 35: 430, 1982.
- Mataizeau J.P., Gayet C., Schmitt M., Prevot L: The
use of free full thickness skin grafts in the treatment of complications of burns. Prog.
Pediat. Surg., 14: 109, 1981.
- Hirshowitz B., Karev A., Rousso M.: Combined double
Z-plasty and YN advancement procedure for repair of thumb web contracture. Hand, 7: 29,
1975.
- El-Ottify M.A.: A versatile method for the relase of
burn scar contractures. Br. J. Plast. Surg., 34: 326, 198 1.
- Salmon I.: "Artères de la peau". Masson
et Cie, Paris, 1936. Cited from Yanai et al., Plast. Reconstr. Surg., 76: 126, 1985.
- Dos Santos L.F.: Le lambeau scapulaire et l'artère
cutanée scapulaire. Mem. Labor Anat. Paris, 1984.
- Dos Santos L.F.: The vascular anatomy and dissection
of the free scapular flap. Plast. Reconstr. Surg., 73: 599, 1984.
- Mayou B_ Whitby D., Jones B.M.: The scapular flap:
anatomical and clinical study. Br. J. Plast. Surg., 35: 8-135 1982.
- Fridlander E, Lee K., Vaudeovord J.G.:
Reconstruction of the axilla with a pectoralis major myocutaneous island flap. Br. J.
Plast Surg., 35: 144, 1982.
|