Annals oj'the MBC - vol. 3 - n 1 - March 1990 SKIN BANK ORGANIZATIONPousa Real F. Serv. de Cirurgia Plastica, Hospital Juan Canalejo, La Coruna, Espaha SUMMARY. A survey is made of the organizational considerations that have to be faced in the setting-up of a skin bank, 1 hesc concern equipment, personnel, records and quality control. The methods of acquiring, processing, preserving and storing the skin are Careful records must be kept of its origin and destination. Strict application of a predetermined protocol will ensure a regular supph oi'~ iable allograft for the plastic surgeon. Concept Personnel The Skin Bank is a service, not a product. It is necessary to leave the processing and banking in the hands of a physician. The methodology requires a close cooperative relationship with the person in Records charge of research. The Skin Bank is a central service, available to the Plastic Surgery Department and especially to the Burns Unit. History The first report on skin freezing was
by Mider and Morton in 1939. In 1945 Strumia and Hodges published the first article on the
freezing of rat skins. Medawar and Wilfingcr published the first article on
cryopreservation, using 14% Gycerol as an anti-freeze. Lher in 1964 established the
relationship between the speed of slow freezing and quick thawing. Randolf May and De
Clement published a series of publications in which they carried out studies on the
viability, contamination and methodology of cryopreservation. Quality control Bacteriological control, viability control, cost control, etc. Acquisition of tissue
The following documentation was utilized when available to obtain information about the donor in order to apply selection criteria:
The potential donor was excluded front use if any of the following conditions were present:
Processing, preservation and storage
1. Timely Collection of Skin Skin allograft collection should be carried out as soon as possible after the death of the donor. The body should be cooled in the morgue refrigerator if collection is to be delayed for more than four hours. Skin should be collected within 10 hours after death. 2. Fluids The solutions used for collection,
processing and storage of the skin should be sterile and isotonic (e.g. M.E.M. 80%, F.B.S.
10%, antibiotic solutions 2%, cryo-protector agents if storage for freezing: DMSO 15%,
Glycerol). 3. Skin Collection Room, Workroom When feasible, skin collection should
be done in a room where environmental contamination can be minimized. Access to the area
should be restricted during skin collection, and other activities -in the immediate area
suspended to cut down on exogenous contamination. 4/5. Preparation and Collection of Skin The body surface is divided into
independent areas for removal and preparation; surgical removal of skin was carried out on
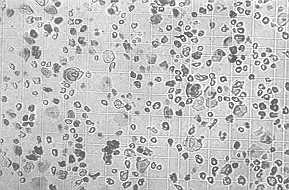
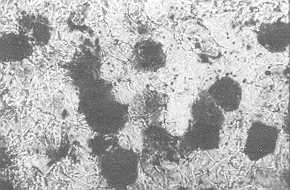
defined areas. 6. Residual microbiological flora evaluation One 1 CM2 full-thickness biopsy from
each of the body areas was minced, and homogenized in 2 ml Of sterile 0.9% NaCI for
microbiological study in the bacteriological laboratory. 7. Packaging and Labelling Final packaging should be done as soon
as possible after collection of skin in a specifically designated "clean area"
or a laminar-flow unit equipped with HEPA filters. Sterile instruments, aseptic procedures
and low temperatures should be used during all stages of processing and packaging to
minimize contamination by micro-organisms and to maintain skin viability. The packaging
materials should be sterile, physically. suitable for the anticipated methods of storage
(e.g. Gambro), inert under the customary conditions (- 186 *Q of use, and sufficiently
scalable to exclude external contamination. Information sheet 1 . The generic name of the product 8a. Storage for Freezing The allograft should be treated with the cryoprotective agent for a sufficient length of time (I to 2 hours) before freezing to ensure adequate protection. Freezing of viable skin grafts should be carried out using a system (freezing chamber TRA-13, microprocessor 8050 PPC-21 and nitrogen container Carburos Metalicos S.A. Espana) which allows a freezing ratio of -1 or -2 'C per min until it reaches -100 V. The microprocessor maintains two registers of temperature, one of the chamber and the other of cryotube control (which is the temperature of the packets of skin). Applying the freezing programme, previously obtained experimentally, the skin is stored submerged under liquid nitrogen in a liquid nitrogen refrigerator (600 1. Carburos Metalicos S.A.) to -180 V. 8b. Storage for Refrigeration Split-thickness skin graft may be stored at 1 'C to 10 'C for several days following acquisition. It is sterile, if appropriate antibiotics have been added to the medium at an effective concentration. The viability of skin not used after one week cannot be assured. 9. Distribution Request for information. The skin bank must request the following information before release of skin for patient use: Request for information 1. Recipient patient's name Distribution documents
Transportation and Use of Frozen Skin The skin should be maintained at or below -70 'C during transportation. Skin should be thawed using procedures which maintain suitable viability. One such procedure is rapid thawing in isotonic solution maintained at 35 'C or 37 'C. After thawing, open packages of skin may be kept at between 1 'C and 10 'C for up to 24 hours. Results and conclusion
RÉSUMÉ. Au moment de créer une banque de la peau il faut tenir compte d'une série de considérations organisationnelles qui concernent l'équipement, le personnel, la documentation et le contrôle de la qualité. Il y a une description des méthodes pour repérer, traiter, conserver et stocker la peau. Il faut documenter attentivement son origine et sa destination. L'observation absolue d'un protocole prédeterminé garantit au chirurgien plastique une provision régulière d'allogreffe viable. |