| Annals qf the MBC - vol. 3 - n' 1 - March 1990
THE USE OF GAMMAGLOBULINS AND
IMMUNOMODULATORS IN THE THERAPY OF INFECTIONS IN SERIOUS BURN PATIENTS
Magliacani G., Stella M.
Centro Traurnatologico di Torino, Divisione
di Chirurgia Plastica, Centro Grandi Ustioni, Torino, Italia
SUMMARY. The causes of
infection in burn patients are examined in relation to origin and type. The importance of
the condition of anergy in these patients is underlined. For correct immunological therapy
it is indispensable to have an accurate diagnosis with haemocultures, biopsies,
lymphograms, etc. On the basis of five years' experience the use is recommended of
gammaglobulins in patients with a low scrum IgG titre in the shock phase and/or sepsis.
Despite the absence of precise evidence regarding the utility of immunomodulators, their
use is ic.cornmended whenever the bacterial flora present is not sensitive to antibiotics
and in the pre-operative phase.
Observations in recent years have
indicated with increasing clarity that local burn lesions can induce in the various organs
and systems a series of efTects which manifest themselves in serious modifications in the
defence mechanisms.
Sepsis, or Multi Organ Failure (MOF) resulting from it, is responsible for 75% of deaths
occurring in burn patients after the emergency phase (1).
The reason for the high death-rate in burn patients is principally the state of
immunodepression and the frequent ineffectiveness of antibiotic therapy due to the
presence of polyantiblotic-resistant bacterial strains.
Although long considered an unavoidable event, infective complications were observed in
only 50% of a series of our cases.
Generally speaking, an infection depends on the interaction between germ, host and
environment; if the relationship of one of these factors with the other two is altered,
conditions may develop that favour the onset of sepsis (2).
In the specific case of the burn, the infective complications can be reduced to three, in
relation to type and origin:
- nosocomial: infections contracted in the hospital
environment from polyantibiotic resistant germs and characterized by the onset of
cross -1 rife ctions, the spread of which is determined by fixed or mobile carriers, for
example the medical staff.,
- iatrogenic: infections caused by invasive diagnostic
and/or therapeutic procedures;
- opportunistic: infections for which normally commensal
germs are responsible.
The observation of opportunistic
infections recalls the concept of the compromised host, i.e. a host with an objective lack
of defence mechanisms against Infection, due to immunodeficiencies.
The deficiencies variously affect susceptibility to infection, in relation to the specific
mechanisms, the degree to which they have been compromised, and the presence of previous
and/or concomitant pathology.
In physiological conditions there are numerous defence mechanisms:
1 - Physical and chemical barriers. These
aye represented by the integrity of the skin and the mucosae, the presence of the
sphincters and the epiglottis, gastric acidity, peristalsis, secretory and excretory
efficiency, and the presence of endogenous microbic flora.
In bum patients we are in the presence of extensive cutaneo-mucosal lesions, sometimes in
the perineal area, bladder catheterization, not infrequent bums of the airways, gastric
acidity disorders, and alterations of the endogenous microbic flora, at both cutaneous and
intestinal level. In the first 48 hours post-bum there is the onset of a more or less
severe enteroparalysis and the intestinal bacteria can easily escape from the intestinal
epithelium and invade the circulation, sometimes taking up location in the burn areas but
always provoking endotoxinaemia (4, 5).
2 - Inflammatory response. Important
elements in this response are the activity of the inflammatory cells, such as the
granulocytes, mediated by humoral soluble products, the complementary cascade, especially
of fractions C3, C4, C9 and C10, and the presence of fibronectin. The bum patient
may present a number of anomalies also in this field: the functions of the PMN phagocytes
are altered, especially during the shock phase and in the course of sepsis, and
complementaemia and fibronectinaemia are constantly low during the shock phase (6, 7).
PATHOGENS CAUSING INFECTION
(Total number of isolations in 1987 = 533) |
STAPHYLOCOCCUS AUREUS Me-R
STAPHYLOCOCCUS AUREUS Me-S
STAPHYLOCOCCUS COAG-NEG
PSEUDOMONAS AERUGINOSA
STREPTOCOCCUS FAECALIS
STREPTOCOCCUS PNEUMONIAE
ACINETOBACTER CALC. ANITR.
ESCHERICHIA COLI
ENTEROBACTER CLOACAE
KLEBSIELLA PNEUMONIAE |
122(23%)
98(16%)
13( 2%)
102(19%)
67(11%)
6( 1%)
35( 7%)
23( 4%)
17( 3%)
13( 2%) |
|
Table 1 |
|
3 - Reticuloendothelial system. This
is mainly composed of tissue phagocytes.
In the bum patient the tissue phagocytes present alterations at the level of phagocytosis
and intracellular killing, modified secretion of inter-immunosuppressors must be
considered in this leukin-I (IL-1) and interferon (IFN), and a reduction of the expression
of MHC-11, making cooperation with The presence of pharmacological and endogenous context.
The latter include serum active peptide (SAP), which suppresses lymphocyte blastogenesis
and inhibits lymphokine synthesis, prostaglandins (PGE2), leukotrienes (LT134),
thromboxans, the trauma-related products of the cyclo- and lipo-oxygenase of arachidonic
acid, which exert a suppressive effect on the mixed lymphocyte culture, and lastly the
degradation products of fibronectin, fibrinogen and collagen, which show activity similar
to that described. above (7, 13). For the determination of the patient's condition other
factors are involved such as hypermetabolism, hormonal imbalances and the presence of
necrotic tissue. A situation of infective susceptibility therefore prevails, which begins
with the loss of cutaneous protection and is facilitated by the presence of an avascular
devitalized tissue, an easy terrain for bacterial colonization; this situation is
explained particularly by the profound metabolic and biochemical disturbances which
characterize the bum illness, and which, all considered, are equivalent to a state of
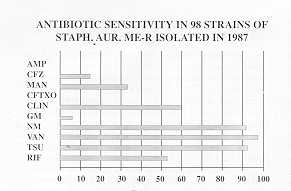
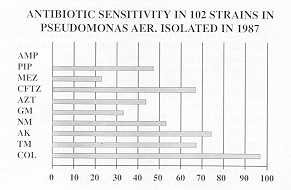
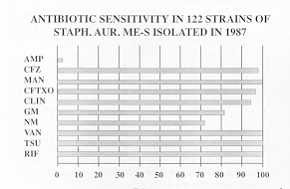
severe damage in the immune system. To complete the picture, mention must also be made of
the bacterial flora present (Table 1), which is often polyantibiotic-resistant (Tables
2-4).
4 - Immune reaction. This
is the specific and aspecific response to the antigenic aggression. The T and B
lymphocytes, with their soluble products, the NL cells, are peculiar to this response.
The most striking characteristic of the burn patient, which has long been known, is the
condition of anergy, demonstrated by the non-rejection of noncompatible allografts, which
may continue for weeks (8).
The data show reduced NK activity in these patients and, with reference to the cooperation
between lymphocytes and macrophages, underproduction of interleukin-2 (IL-2) and its
receptors, which is a conditioning factor for the clonal expansion of the lymphocytes (7,
9). Alterations have been described in the T-line subpopulations, with an increase of T
suppressors, suggesting the T4/T8 relationship as a suppression index; however there is
insufficient confirmation of these data (7, 10, 11).
We found in the cases we observed that the development of the disease frequently did not
proceed parallel to the behaviour of the T lymphocytes. To be more precise it was found
that a high T suppressor rate was not accompanied by serious septic episodes and that
important infections often occurred in patients with a low T suppressor rate, throwing
doubt on the diagnostic value expressed by the T4/T8 relationship.
The use of double marking enabled us to observe that a global increase in T8 corresponded
to an increase in cytotoxics rather than in suppressors and that the reduction in T4 was
to be correlated with a reduction in the inductors. It was also found that clinical
development was favourable in patients with a considerably impaired T4/T8 relationship but
with physiological helper and suppressor conditions, and unfavourable with a regular T4/T8
ratio accompanied by vast disproportions between helpers and inductors and/or suppressors
and cytotoxics.We therefore believe that a number of data still used today in diagnostics
should be reviewed and above all reinterpreted, at least with reference to cellular
competence.
Another common finding is a more or less marked depletion of IgG in the shock phase; B
lymphocytes in burn patients, isolated in vitro, showed an aspecific polyclonal
production of immunoglobulins, which could be correlated with the patients' late
hypergammaglobulinaernia, but which might also indicate poor specificity of the response
(12).
The burn patient therefore constitutes an extremely complex case of an infective-risk
host, whose treatment must be completely rational if the means available are to be
successful.
Our experience has shown that it is useful to classify the patients in homogeneous groups
according to their clinical situations and infective risk. We chose an index that takes
into account the extent and depth us to group the patients in five risk classes within
which it was possible to obtain comparable situations with regard to mortality, sepsis
rate, hospitalization times and the duration periods of the intravenous line and the Foley
catheter (14).
It was found that infection increased in frequency and complexity (mono- and polymicrobic)
as the risk class increased (Table 5) and that, for example, in patients belonging to the
first class, systemic antibiotic therapy could be discarded as a method, as topical
treatment proved to be sufficient treatment. As the success of the treatment is due above
all to a correct and aimed therapy, it is indispensable to have accurate diagnostics with
absolutely reliable tests, such as haemoculture, biopsies examined with microbiological
and histological methods, the bactericide power of serum and the lymphocytogram.
DISTRIBUTION OF
INFECTIONS ACCORDING TO RISK CLASS
| |
I |
II |
III |
IV |
V |
MONOBACT. |
17 |
4 |
3 |
4 |
1 |
POLYBACT. |
7 |
7 |
4 |
8 |
6 |
TOTAL |
24 |
11 |
7 |
11 |
7 |
|
Table 5 |
|
With reference to problems of
immunological deficiency, we observed in the shock phase constantly low IgG titres, which
began to recover from the second week, and sometimes late- hypergammaglobulinaemia.
It is considered an unfavoui-4ble prognostic sign if low IgG values persist beyond the
initial period.
Correction of this situation with gammaglobulins does not appear necessary, just as we
believe that the administration of IgG to all patients as a preventive measure is not
useful.
The use of this therapeutic technique in burn patients must in our opinion be limited to
precise indications and in comparable situations.
In the light of our five years of experience we suggest that substitutive gammaglobulin
treatment should be initiated only in the presence of particular conditions, considering
that the preventive use of high doses in all patients did not give the expected results.
At present we use gammoglobulins only in the presence of a low IgG scrum titre during the
shock phase (due to extravasal losses), of sepsis (due to detrition), and of septic shock,
administering i.v. between 500 and 1000 mg/kg body weight.
Following these indications, the use of IgG improved the chemotaxis index and the opsonic
activity of the serum, and reduced endotoxaemia. Clinically speaking, this meant a
reduction in mortality and an improvement in the prognosis of sepsis; however septic
events were neither totally prevented nor even significantly reduced in number (7, 15).
The theoretical justification for the use of immunomodulators (thymostimulins and
thymopentin) is based on the demonstration that these substances stimulate the maturation
of lymphocytes originating in the thymus, both physiologically and in certain diseases of
the immune system in which these cells are compromised.
Although there is no conclusive evidence regarding the use of these immunomodulators in
burn patients, we believe that this is the correct approach in situations in which the
patient's clinical state does not seem to improve with other therapies, when for example
the bacterial flora is not sensitive to the antibiotics available or when, despite in
vitro sensitivity, the results obtained are unsatisfactory. Immunomodulators should also
be used in the pre-operative period.
Using thymostimulin we administer doses of 1-1.5 mg/kg every day in the first week, and on
alternate days in the following 3-4 weeks. Using thymopentin we administer 50 mg on
alternate days; for 3-6 weeks.
The limit to the rational use of immunologic drugs is constituted by the difficulty of
demonstrating the immune state of the bum patient with absolute certainty, with correct
identification of its deficient sectors, and of verifying after therapy the return to a.
normal state.
However, we believe - until contradictory evidence is presented - that if the above
indications are followed the use of gammoglobulins and of immunomodulators may represent a
further therapeutic possibility in the various techniques available in the treatment of
infection in the severe bum patient.
RESUME. Après avoir traité
les causes de l'infection chez les brûlés pour ce qui concerne l'origine et le type, les
Auteurs considèrent le phénomène de l'anergie qui se manifeste chez ces patients. Ils
soulignent que pour mettre en train une thérapie correcte il faut un diagnostic précis
avec l'hémoculture, la biopsie, le lymphogramme etc. Sur la base de cinq ans
d'expérience, ils conseillent l'emploi des gammaglobulines chez les patients avec un
titre bas d'IgG sérique en phase de choc et/ou de septicité. Malgré l'absence
d'évidences précises pour ce qui concerne l'utilité des immunomodulateurs, les Auteurs
en conseillent l'emploi quand la flore bactérienne chez le patient n'est pas sensible aux
antibiotiques et aussi pendant la phase préopératoire.
BIBLIOGRAPHY
- Pruitt B.A. Jr.: The diagnosis and the treatment of
infection in burn patients. Bums, 11: 79-91, 1984.
- Dionigi R., Colombo D.H., Nazari S., Grassi M.,
Boriolo P.: 11 trattamento delle infezioni nel periodo postoperatorio di pazienti ad alto
rischio. Min. Chir., 37: 1-15, 1982.
- Gelfand J.A.: Infection in burn patients: a paradigm
for cutaneous infections for the patient at risk. Am. Med.: 138-165, 1984.
- Deitch E.A., Berg R.D.: Endotoxin but not
malnutrition promotes bacterial translocation of the gut flora in burned mice. J. Trauma,
27: 161-166. 1987.
- Deitch E.A., Berg R., Specian R.: Endotoxin promotes
the translocation of bacteria from the gut. Arch. Surg., 122: 185-190, 1987.
- Winkelstein A.: What are the immunological
alterations induced by burn injury? J. Trauma, 24: 72-80, 1984.
- AA.VV.: Abstracts of the First International
Congress on the Immune Consequences of Trauma, Shock and Sepsis. Munich, 11~988.
- Dogo G.: "Chirurgia plastica
ricostruttiva". Padova CLEUP, 1972.
- Teodorczuk J.A., Sparkes B.G., Mills G.B.:
Impairment of T cell activation in burn patients: a possible mechanism of thermal
injury-induced immunosuppression. Clin Exp. Immunol., 65: 570-581, 1986.
- Antonacci A.C., Goor R.A., Gupta S.: T cell
subpopulations following thermal injury. Surg. Gyn. Obst., 1: 155-160, 1982.
- Magliacani G., Stella M: Immunologia e ustioni. Atti
36 Congr. Naz. Soc. It. Chir. Plast., 231-234, 1987.
- Teodorczyk J.A., Sparkes B.G., Falk R.E., Peters
W.J.: Polyclonal immunoglobulin production in burned patients. Kinetics and correlations
with T cell activity. J. Trauma, 26: 834-839, 1986.
- Constantian M. B.: Association of sepsis with an
immunosuppressive polypeptide in the serum of the burn patients. Ann. Surg., 188: 209-213,
1978.
- Soranzo M.L., Stella M., Pizzo L., Daziano F.:
Considerazioni sulla sorveglianza clinico epidemiologica in reparto per Grandi Ustionati.
Atti 36 Congr. Naz. Soc. It. Chir. Plast., 341-344, 1987.
- Muster A.M., Winchurch A.R., Moran A.T.:
Prophylactic intravenous immunoglobulin replacement in high risk burn patients. Atti
Congr. Immunodeficiencies and Autoimmune diseases, Venice, 1987.
|