Annals of the MBC - vol. 3 - n' 2 -
June 1990
MICROSURGICAL
TREATMENT IN ACUTE BURNS AND THEIR SEQUELAE
Lorenzini M., Cristofoli C., Governa M., Rigotti
G., Barisoni D.
Divisione di Chirurgia Plastica e Centro Ustioni, Verona,
Italia
SUMMARY. The development
of microsurgery techniques over the past years has enabled us to obtain striking results
in difficult cases which were not easily treated years ago. In burns therapy microsurgery
has introduced a new philosophy of therapeutical approach, both in the acute phase and in
the treatment of sequelae. The Authors present the experience of the Verona Burns Centre,
Italy, with these innovative techniques, showing possible applications and describing
cases. The results are excellent, but it is stressed that the patients have to be
carefully selected. An analysis is made of the advantages that these methods can ofFer in
comparison to traditional techniques.
Introduction
Microsurgery in burns therapy has
certainly offered surgeons a new and effective way of solving several critical problems.
It has precise indications both in the acute phase and in the treatment of sequelac,
according to the conditions and limitations of this kind of surgery.
First of all we have to consider:
- the general conditions of the patient, who will be
subjected to a long general anaesthesia, and the viability of his local and general
vascular situation;
- the real advantages we may gain with these particular
techniques, without disregarding the traditional methods which are always to be considered
as the first choice;
- the availability of well-trained and experienced medical
staff in order to minimize the risk of failures.
Acute burns
In acute burns, microsurgery finds a
well-defined indication in the treatment of localized full-thickness lesions with exposure
of important structures, such as tendons, bone and nerves. It allows us to cover these
tissues with viable and well-vascularized flaps that offer immediate protection from the
risk of infection and further necrosis; the forearm, hand, ankle and foot are the most
common recipient areas.
When choosing the flaps, we have to estimate the size of the lesion and the functional and
aesthetic characteristic of the area, dissecting a flap of suitable size and thickness.
Burns sequelae
In burns sequelae, microsurgery offers
interesting solutions for the treatment of scar contractures and disfiguring scars in all
those areas like limbs and face, where customary techiques seem to give insufficient
results. Free flaps allow us to replace the damaged surfaces with soft, viable tissue
which, in addition to a satisfactory cosmetic result, often gives functional recovery too.
For these reasons, particular attention has to be made when choosing the flap, assessing
its matching with the recipient area, size and thickness, and considering the residual
damage in the donor site.
Material and method
In Verona, we have treated 16 cases using
microsurgical reconstruction: 9 in the acute phase and 7 for improvement of severe burns
sequelae. Electrical and contact burns were the most common acute lesions in our series
(Tab. 1).
| Type of burn |
acute |
sequelae |
| Electrical |
4 |
- |
| Chemical |
- |
1 |
| Flames |
- |
5 |
| Contact |
5 |
1 |
| Total |
9 |
7 |
|
| Tab. 1 CLINICAL SURVEY 16 CASES |
|
Microvascular sutures were performed with
nylon 9/0 or 10/0, arteries were usually connected by end-to-side suture and veins
end-to-end.
The flaps used in our 16 patients and the recipient sites are reported in Tab. 2.
| Flap |
upper limb |
lower limb |
face |
| Latissimus D. |
1 |
- |
- |
| Scapular or parascapular |
6 |
2 |
- |
| Dorsalis P. |
4 |
- |
1 |
| Temporalis F. |
1 |
1 |
- |
|
| Tab. 2 FLAPS USED AND RECIPIENT AREAS |
|
Results and discussion
We had only one failure, in a patient with
a deep electrical injury in the left wrist, due to a venous thrombosis correlated to the
local vascular condition.
 |
 |
 |
Case 1: A) Severe
burn sequelae of the left hand B) Dorsal pedis free laps C) Satisfactory
functional result |
|
In all the other cases we obtained
satisfactory results with sufficient cosmetic and good functional recovery.
Different flaps were performed according to the needs of the various recipient areas and
the characteristic of the different donor sites (Tab. 2).
Dorsalis pedis flaps were preferred in the treatment of lesions of the hands and face
(cases 1 and 2), while larger and thicker flaps such as scapular and parascapular find
their best utilization in the forearm, wrist and ankle (case 3).
With the progress and refinement of microvascular techniques, it has become possible to
solve several critical problems in the surgical treatment of burned patients. Both in the
acute phase and in burns sequelae this treatment seems to be the best remedy in more
severe injuries.
Nevertheless traditional techniques remain the first choice in most cases, offering easier
and equally effective solutions. Furthermore, thanks to the utilization of skin expanders,
it is possible to obtain wide and movable local flaps which now appear to be the best
solution in the treatment of scar contractures in particular areas like the neck and
armpit. For these reasons, an accurate evaluation of all available surgical techniques and
of the patients' general and local conditions is the first step in any logical
microsurgery programme.
 |
 |
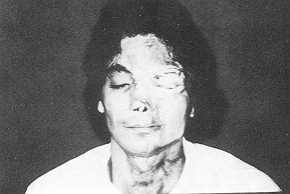 |
Case 2: A)
Disfiguring scars of the face B) C) The result after partial
reconstruction with dorsalis pedis free flap |
|
 |
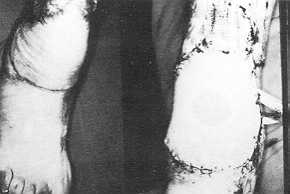 |
| Case
3: A) Deep bum of the ankle with tendon exposure B) Coverage
with scapular free flap |
|
RESUME. Le développement des techniques de
la microchirurgie dans ces dernières années nous a permis d'obtenir des résultats
exceptionnels chez certains patients que nous pouvions soigner seulement avec grande
difficulté il y a très peu. Dans la thérapie des brûlures la microchirurgie a
introduit une,nouvelle philosophie d'approche thérapeutique, pour ce qui concerne soit la
phase aiguë soit le traitement des séquelles. Les Auteurs présentent l'expérience du
Centre des Brûlés de Vérone, Italie, avec l'emploi des techniques innovatrices. Les
résultats ont été excellents, mais il faut toujours sélectionner les patients avec
grande attention. Les Auteurs analysent les avantages de ces méthodes par rapport aux
techniques traditionelles.
BIBLIOGRAPHY
- Baik B.S., Kim 1.K.: Reconstruction of the burned
lower extremities by free flaps. Eur. J. Plast. Surg., If: 17, 1988.
- Barwik W.J., Goodkind D.J., Serafin D.: The free
scapular flap. Plast. Reconstr. Surg.: 779-787, 1982.
- Brent B., Upton J., Acland R.D. et al.: Experience
with the temporoparietal fascia free flap. Plast. Reconstr. Surg., 76: 177-188, 1985.
- Brunelli G.: Free skin flaps. Generalities.
-Textbook of Microsurgery", 111- 116, Masson, Milan, 1988.
- Daniel R_ Taylor G.l.: Anatomy and hemodynamics of
free' flap donor sites. Symposium on Microsurgery, 32-40, Mosby, 1976.
- Harii K., Ohmori K.: Free skin flap transfer. Clin.
Plast. Surg., 13: 111-127, 1976.
- Ikuta Y.: Free flap transfers by end to side
arterial anastomosis. Br. J. Plast. Surg., 28: 1, 1975.
- MeCraw J.B., Furlow C.T.: The dorsalis pedis
arterialized flap. A clinical study. Plast. Reconstr. Surg., 55: 177, 1975.
- Nassif T.M., Vidal L., Bovet J.L., Baudet J.: The
parascapular flap: a new cutaneous microsurgical free flap. Plast. Reconstr. Surg., 64:
591-600, 1982.
- Ohmori K., Harii K.: Free dorsalis pedis sensorial
flap to the hand with microneurovascular anastomosis. Plast. Reconstr. Surg., 58: 546,
1976.
- Rigotti G.: Donor site pathology in the free
microvascular grafts. "Textbook of Microsurgery", 125-130, Masson, Milan, 1988.
- Rigotti G. et al.: 11 lembo libero microvascolare
dorsale del piede. Riv. Ital. Chir. Plast., 699: 16, 1984.
- Song R., Gao Y., Song Y., Yu Y.: The forearm flap.
Clin. Plast. Surg., 9: 21-26, 1982.
- Watson J.R., et al.: The free latissimus dorsi
myocutancous flap. Plast. Reconstr. Surg., 64: 299, 1979.
|