Annals of the MBC - vol. 3 - n' 2 -
June 1990
EARLY NEUROLOGICAL
COMPLICATIONS IN ELECTRICAL BURNS
Haberal M., Bayraktar U., OztOrk S., Oner 1, Bilgin N.
Hacettepe University Hospital, Ankara, Turkey
SUMMARY. It
was observed that high-tension electrical burns rnay cause major damage to the neural
system, even in the absence of severe tissue injury. A description is given of three
such patients, who suffered variously from loss of sensation, myelopathy, a
paraplegia-like syndrome and neuropraxia. It is therefore advisable to perform a thorough
neurological examination in patients with electrical burns, even if they do not present
severe tissue injury, in order to prevent later complications.
Introduction
Burn therapy has long been a major
problem in Turkey and the therapy of electrical bums in particular requires special
attention.
In our country, electrical energy is used widely but sometimes inappropriately. For this
reason, the incidence of this type of bum, which causes severe complications or death, is
considerably high. On average, 15% of the patients admitted to our Burn Unit are diagnosed
as having electrical bums (1).
In this series we have observed that the high tension of electrical burns can cause major
damage to the neural system, though not causing any severe tissue injury.
Materials and methods
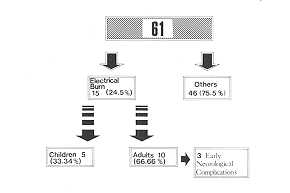
From Ist January 1988 to 31st December
1988 61 burned patients were admitted to our Burn Centre. 15 (24.5%) presented electrical
burns (Fig. 1). Three of the adult patients had early neurological complications without
displaying any severe tissue damage. All three patients were hospitalized in our hospital
or another centre following the injury.
Case 1: A 40-year-old male electrician came into contact with a high-voltage
electricity supply (30,000 volts) while working. Electrical current entered through his
neck and exited from the bilateral hands. On admission, physical examination showed 25%
TI1SA burns (23% second-degree and only 2% third-degree).
The burns area included: back of body (superficial second-degree) 14%, front of the body
3%, left hand 1%, right hand 1%, left leg 2%, neck 2%. The patient was treated with our
routine protocol. He did not show any problem with the related kidney but presented
imbalance and there was loss of sensation in the lower part of the back of the body and
the bilateral lower extremities. The neurological examination myelopathy. In exercise was
complications. after admission
Case 2: A 37-year-old male electrician came into contact with a high-voltage
electricity supply (15,000 volts). On admission, physical examination showed 12% T13SA
burn (10% second-degree and 2% third-degree) without revealing any severe tissue damage,
together with 10% burn in the right hand and 11% in the left lower extremity. Electrical
current entered through the right hand and exited from the left lower extremity. Following
the injury, the patient was treated in one of the Community Hospitals and 15 days later he
was transferred to our Centre with a paraplegia-like syndrome. Neurological examination
and EMG showed myelopathy, and vascular damage was diagnosed in the spinal cord. Besides
the burn treatment, physical therapy was applied and the patient was discharged 90 days
after admission, having been advised to continue the physical exercise.
Case 3: A 33-year-old male electrician came into contact with a high-tension
electrical supply (30,000 volts). On examination the patient showed 2 1 % T13SA (18%
second-degree and 3% third-degree), without displaying any severe tissue damage. The entry
point of the electrical current was the left hand and exit was from the left lower
extremity. The burn area was 6% front of body, 2% left arm and 13% left lower extremity.
Following the injury, the patient was treated in one of the Community Hospitals and 48
hours later he was transferred to our Centre. During the treatment he presented loss of
sensation in the bilateral upper extremities. The neurological and EMG examinations showed
bilateral ulnar and median nerve neuropraxia. The patient started physical therapy besides
the bum treatment and he and electromyelography showed addition to the burn treatment,
recommended for neurological The patient was discharged 55 days was discharged on the 7 1
st day following hospitalization, having been advised to continue the physical exercise.
Discussion
Electrical injury is still one of the
main problems in our society in spite of training and prevention activities. Approximately
15% of hospitalized burn patients still present electrical burns (1). Electrical current
mainly travels along the path of the least resistant tissue, such as nerve, vessels,
muscles etc. Electricity can cause injury to the body in three ways. First, electrical
energy can be converted into light, which can damage the eye. Second, the passage of
electrical current through the body can produce effects particularly on the heart and
brain, as a result of which electrical shock occurs. Third, injury May occur by the
conversion of electrical energy into heat. If this occurs outside the body, it causes a
flash burn. If this conversion takes place within the body, a great amount of heat is
produced in the bone where electrical resistance is high (2). The tissue damage will be
high, for the extent of damage is related to the sensitivity of the tissue to heating: in
other words, the least resistant tissue suffers the least severe tissue damage. In
contrast, highly resistant tissue suffers severe tissue damage. Therefore, following
severe electrical injury, approximately 35% of patients have severe musculo-skeletal
complications (3). In spite of severe musculo-skeletal complications, neurological
complications were not a severe problem either in our series or in the literature, in
which very few cases have been reported (4, 5). Most relate to spinal cord injury.
The pathophysiology of electrical spinal injury is as yet unclear and various possible
modes are reported in the literature, such as thermal injury occurring because of heat
production by an electrical current, vascular damage causing thrombosis or haemorrhage,
direct mechanical trauma from fracture or dislocation resulting from intense muscle spasm,
and radiation light effect caused by changes in tissue protein which may lead to secondary
vascular changes (4). In our four cases, we were not able to find out which of the
above-mentioned path ophysiological changes was the cause of the pathology. But this
patient did have a spinal cord injury. Diagnosis was very important for him. Accordingly,
whenever electrical injury patients are admitted to hospital, besides the routine
examination, a neurological examination should also be performed, including ENIG. In
addition to the burn treatment, physical therapy was applied to prevent later
complications.
The evidence obtained from this study supports the view that high-tension electrical burns
can damage the neural system without causing any severe tissue injury. Therefore,
electrical burn patients require close monitoring also of the neurological aspect.
|
Fig. 1 Analysis of 61
patients with respect to burn causes. |
|
RÉSUMÉ. Les Auteurs ont observé
que les brûlures électriques à haute tension peuvent produire des dégâts tissulaires.
Ils décrivent trois de ces patients, qui ont manifesté différemment la perte de
sensibilité, la myélopathie, un syndrome qui ressemble à la paraplégie, et la
neuropraxie. Il est donc conseillable de faire un examen neurologique exhaustif chez les
patients avec brûlures électriques, même s'ils ne présentent pas de dégâts
tissulaires graves, afin de prévenir les complications successives.
BIBLIOGRAPHIE
- Haberal M., Oner Z., Giilay H., Bayraktar U., Bilgin
N.: Severe Electrical Injury and Rehabilitation. Annals of the MBC, 1: 121-123, 1988.
- Gordon M.W.G., Gordon, W.H., Awwaad A.M.: Electrical
Burns - Incidence and Prognosis in Western Scotland. Burns, 12: 254-259, 1986.
- Haberal M.: Electrical Burns: A Five-year
Experience, 1985 . Evans Lecture. The Journal of Trauma, 26: 103-109, 1986.
- Kanitkar S., Roberts A.H.N.: Paraplegia in an
Electrical Burn: A Case Report. Burns, 14: 49-50, 1988.
- Koller J., Orsdg J.: Late Neurologic Sequelae of
High-Voltage Electrical Burns. Abstract Book of IBSI, 58, 1988.
|