Annals of the MBC - vol. 3 - n* 2 -
June 1990
THE USE OF
SALICYLATE VASELINE IN THE DEBRIDEMENT OF BURNS
Maviglio R, Mavilio D., De Donno G., Rume D.
Ospedale Regionale, Divisione di Chirurgia Plastica e
Centro Ustioni, Brindisi, Italia
SUMMARY. Although surgical
escharectomy is the generally accepted method of choice for the elimination of bum
eschars, particular conditions may exist when this technique is not possible. It is
therefore necessary, in order to avoid the risk of septic complications, to remove the
eschar by other means. Salicylate vaseline was used for this purpose in over 500 patients
over a period of 15 years with good results. This ointment has no limitations, and it also
has the advantage of being easy to apply, apart from being inexpensive and easy to
prepare.
Introduction
In this short paper - the fruit of
long experience - we wish to offer our contribution to the solution of one of the most
complex problems encountered in the treatment of the severely burned patient: the
debridement of necrotic areas.
With adequate hydroelectrolytic resuscitatory treatment it is rare to observe deaths in
the days immediately following the bum trauma, whereas towards days 15/20 severe septic
complications may set in, favoured by the presence of considerable immune depression and a
liquefying eschar which constitutes excellent growth pabulum for germs.
These complications are the most frequent cause of patient deaths. It is evidently of
great importance to eliminate the necrotic tissues and to re-cover the patient as soon as
possible.
We too are convinced that early surgical necrectomy must be the method of choice. However
it is very often impossible to bring the patient to the operating theatre, for a number of
reasons - the gravity and the extent of the burns, the serious anaesthesiological risk in
connection with the operation, the presence of airway lesions and last but not least the
difficulty of distinguishing at such an early stage truly necrotic zones from others that
are still viable.
These considerations make it necessary to have at our disposal valid alternative methods,
and many researchers are still today looking for a chemical compound capable of
accelerating the elimination of skin necroses.
Ideally, the characteristics of such an agent are that it should prevent later blood loss
during its debriding action
- be non-toxic for the patient
- be able to remove necrotic tissue without damaging viable
tissue not increase the rate of infective complications not,compromise subsequent graft
take.
In past years Travase was widely used.
This is a substance of enzymatic nature extracted from Bacillus Subtilis which allows
rapid elimination of the eschar (in about 8 days); Travase has however been much
criticized because its use leads to an increase in infective complications (although this
was denied by V. Pennisi, the first proposer of the method) and because it is possible to
treat at one and the same time only limited burned body surface areas (no more than 15%).
We have long been interested in salicylic acid, an agent that is already well known to
dermatologists for its notable keratolytic properties; by acting on the junction between
necrosis and healthy tissue it causes the lysis or loosening of the elastic fibres, of the
bridges of residuous collagenous tissue, and of the coagula and thrombi of fibrin, thus
accelerating its elimination. In addition to this activity salicylic acid also has
bacteriostatic and germicide properties.
Salicylic acid, applied in the medium of white vaseline, can be better distributed over
the surface to be treated and absorption by the tissues can be controlled by modification
of its concentrarion.
This absorption in our experience does not lead to pathological accumulations: we have
never seen a case of serious intoxication due to salicylic acid. This may occur as a
result of an excessive accumulation of high doses. The toxic symptoms (see Table),
although they may be related to the concentration of salicylic acid in the serum, present
a certain individual variability. Clinical and pharmacological studies have however
demonstrated that toxic symptoms do not appear in the presence ot- scrum concentrations
lower than 15 mg/%, appear rarely in concentrations lower than 30 mg/%, and usually occur
in concentrations over 50 mg/%.
Clinical applications
We use salicylate vaseline from day
3/4 post-burn in concentrations varying from 5 to 20%. The concentration depends on the
site, the depth and the type of burn.
In intermediate second-degree burns of the face we use 5% concentrations, spreading the
ointment directly on the lesions, using the method described; the wound is delicately
dressed every day with physiological solution. Debridement occurs gradually and is
complete by day 10, with the spontaneous presence of ample reepithelialization zones and
the absence of excessive secretions and infections.
In intermediate-deep second-degree burns and in third-degree burns caused by hot water we
generally use 10- 15% concentrations, especially when the burn area exceeds 20%.
In third-degree flame burns we use 20% vaseline, after performing some escharectomic
incisions. We apply the salicylate vaseline, spreading it on greased gauze and using
occlusive bandages. The dressing is changed every other day, if necessary with the
assistance of balneotherapy. After about 4 dressings the progressive loosening of the
necrosis becomes evident and is complete on about day 14. On about days 10/12 the eschar
begins to detach itself (Fig. 1) and, similar to wet cardboard (Fig. 4), it is easily
removed with forceps and blunt scissors (Fig. 2); the underlying tissue bleeds very little
(Fig. 3), and the pain is tolerable so that the patient has to be sedated only in the case
of extensive lesions.
The debrided areas are covered with pig skin (E-Z derm) and when the cleansing procedures
are complete they are placed under packs of physiological solution mixed with the
antibiotic that has proved to be sensitive to the antibiogram which we regularly perform
every 3 or 4 days after the patient's hospitalization.
 |
Fig. 1 Third-degree
bums in 25% body area: day 11, initial detachment of eschar. |
 |
Fig. 2 Same
case, day 13: eschar removed with scissors and forceps. |
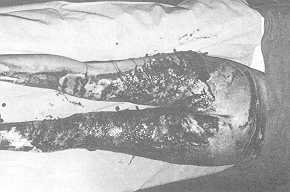 |
Fig. 3 Same
case: . appearance of granulating surface after escharectomy. |
|
It is generally possible to operate on the
patient between day 20 and day 22 (Fig. 5). The take of the graft and the subsequent scar
are both good, and are not unlike the results obtained with surgical escharectomy.
During treatment we naturally monitor the degree and nature of any infections, which are
controlled by aimed antibiotic therapy by general means. The patient is placed on a
Clinitron airbed, if available, and all therapeutic measures are performed that are
necessary for the optimal course of the disease. The monitoring must be watchful for
salicylaemia and the appearance of any clinical signs of intoxication.
 |
 |
| Fig. 4 Same
case: "wet cardboard" appearance of removed eschar. |
Fig. 5 Same
case, day 22: patient ready for operation. |
|
Results and conclusions
We have used the method described with
good results for over 15 years in over 500 patients with severe bums with over 20% BSA in
adults and over 10% in children. On the basis of this wide experience we can make the
following affirmations: the method is easily handled and has no limitations of any kind;
debridement occurs in about 14-16 days with the formation of a good granulation tissue
which is ready to receive the graft on day 20-22; the patients are discharged after 35-40
days of hospital treatment.
Salicylate vaseline does not seem to affect bacterial growth or provoke an increase in
infections, and salicylaemia was always maintained under values of 30 mg/%; the rare cases
of initial intoxication were satisfactorily treated by simply suspending the application
of salicylate vaseline.
Last but not least, one consideration should not be neglected: the low cost of the
ointment, which is prepared directly in the hospital pharmacy.
Table
Symptoms of salicylism
- initial:
- subsequent:
- nausea, vomiting, diarrhoea, disturbances of the sight,
momentary mental aberration
- advanced:
- mental confusion, excitement, talkativeness, restlessness,
respiratory alkalosis
RÉSUME. Bien que l'excision chirurgicale
soit la méthode généralement préférée pour l'élimination des escarres des
brûlures, cette technique n'est pas toujours praticable, à cause de conditions
particulières. En ce cas, pour éviter le risque des complications septiques, il faut
détacher l'escarre en manière diverse. Pour atteindre ce but, les Auteurs ont utilisé
la vaseline salicylée chez plus de 500 patients dans une période de plus de 15 ans, avec
de bons résultats. Cet onguent n'a pas de limitations, il a l'avantage d'être facile à
appliquer, il coûte peu et sa préparation est aisée.
BIBLIOGRAPHY
- Connell J.F., Rousellot L.M.: The use of enzymatic
agents in the debriding of burn and wound sloughs. Surgery, 30: 53, 195 1,
- Davies M., Marks R.: Studies on the effect of
salicylic acid on the normal skin. Br. J. Derm., 95: 187, 1976.
- Goodman L.S., Gilman A.: "The pharmacological
basis of therapeutics", Macmillan, 1975.
- Huber C., Christophens E.: Keratolytic effect of
salicylic acid. Arch. Derm. Res., 257: 293, 1977.
- Hummel M.P., Kauts P.D., Macmillan B.G.: The
continuing problems of sepsis following enzymatic debridement of bums. J. Trauma, 14: 572,
1974.
- Jackson D.M., Stone P.A.: Tangential excision and
grafting of burns. Br. J. Plas. Surg., 25: 416, 1972.
- Janzekovic Z.: Excision of bums. Burns, 4: 1, 1977.
- Levick P.L., Brough M.D., Vasilescu C.T. et al.:
Treatment of full thickness burns with Travase: result of clinical trial. Bums, 4: 281,
1978.
- Makepeace A.R.: Enzymatic debridement of bums: a
review.Bums, 9: 15~, 1983.
- Masellis M., Vitale R., laia A.: Surgical and
chemical necrectomy: two methods for debridement of the burn wound. Riv. It. Chir. Plast.,
13: 17, 1981.
- Maviglio P., De Santis P., Marasco L. et al.: The
utilization of salicylic vaseline in the debridement of burns. Riv. It. Chir. Plast., 13:
37, 1981.
- Pennisi V.R., Capozzi A., Friedman G.: Travase, an
effective enzyme for bums debridement. Plas. Reconstr. Surg., 51: 371, 1973.
- Pennisi V.R., Abril F., Capozzi A.: The combined
efficiency of Travase and Silver Sulphadiazine in the acute burns. Bums, 2: 196, 1976.
- Shakespeare P.G.: The activity of the enzymatic
debridement agent Travase towards a variety of protein substrates. Bums, 6: 15, 1979.
- Singh G.B., Snelling C.F.T., Hogg G.R. et al.:
Debridement of the bum wound with smilains ointment. Bums, 7: 41, 1980.
- Taylor J.R., Halpring K.M.: Percutaneous absorbtion
of salicylic acid. Arch. Dermatol., 3: 740, 1975.
- Weirich E.: Dermatopharmacology of salicylic acid.
Dermatologica, 151: 268, 1975.
- Weirich E., Longauer J.K., Kirkwood A.H.:
Dermatopharmacology of salicylic acid. Dermatologica, 152: 87, 1976.
|