Annals of the MBC - vol. 3 - n' 2 - June 1990 TOLERANCE AND COMPLICATIONS OF EARLY ENTERAL NUTRITION IN BURNSloannovich J., Llakakos Th., Panayotou P., Mantas N., Alexakis D. Center of Plastic Surgery and Microsurgery, General State Hospital of Athens, Greece SUMMARY. Total enteral nutrition (TEN) following bum injuries has been used in clinical practice only in the past two years, and there is still some scepticism about its validity. It is widely believed that TEN should commence only after the 3rd day post-burn, because of the danger of paralytic ileus. A study was carried out to evaluate the tolerance of early TEN after bum lesions and to investigate its clinical and biochemical side effects. In three groups of patients (total number 13, average age 45 yrs, T13SA 20-75%), TEN was initiated respectively in the first hours post-burn, on the first day post-burn, and between the 2nd and the 5th day post-bum. The results obtained showed that TEN was satisfactorily tolerated, without major gastric or intestinal side effects or irreversible side etTects on the hepatic tissue. All side effects were mild and were resolved without difficulty. Morbidity was low because of the improvement in the patients' general conditions, the absence of upper G.I. tract bleeding and the reduction in septicaemia. Mortality was also significantly reduced. The TEN technique can therefore be said to be well tolerated, irrespective of the time of its initiation. Introduction Total enteral nutrition (TEN) tends to become the treatment of choice in burns, since there is experimental and clinical evidence that it diminishes the incidence of complications and ameliorates the outcome of burn victims (Wilson 1975, Moss 1975, Kirksey 1968). Since the clinical experience of using TEN is just two years old, possible side effects still create scepticism about its mode of use (Alexander et al. 1984, McArdle 1984, loannovich et al. 1989). In our bum unit we decided to evaluate the tolerance of early TEN and investigate its clinical and biochemical side effects. In this way we try to give an answer to two crucial questions:
Material and methods In 1988 13 patients were studied (Tab. 1). Their average age was 45 yrs and the extent of their bums ranged from 20-75% TI1SA. According to the initiation of TEN, three groups were formed (Tab. 2). In Group A (n=5), nutrition commenced in the first post-burn hours. In Group B (n=4) nutrition commenced on the first post-burn day and in Group C (n=4) nutrition commenced between the 2nd and 5th post-bum day, since patients in this group were transferred to our unit after a period of delay.
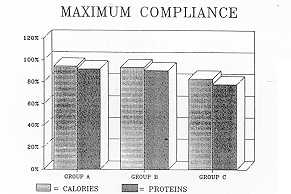
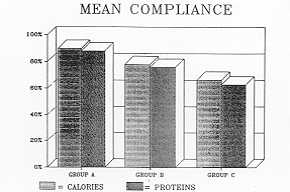
On admission a fine radiopaque nasoduodenal tube was inserted in all patients. An enteral nutrition pump for continuous and controlled administration of a semielemental enteral solution was used. The solution contains 17.5% of energy as hydrolysed proteins (Tab. 3). The initial infusion rate was 25 ml/h and was gradually increased by 25 ml/h every 12 h, until the calculated amount was reached. TEN was terminated by the completion of wound healing. The calculation of nutritional needs was performed -according to the Davies Li1jendahl formulae, up to 45% TBSA (Tab. 4). Besides the initial calculation, nutritional needs were recalculated at the end of the first post-burn week and from then on, every ten days, according to the reduction of the TBSA. In an attempt to investigate the tolerance of early TEN, the G.I. tract and hepatic behaviour, together with the mean and maximum compliance, were used as indices.
To complete our study on tolerance, it was necessary to examine the morbidity and mortality of this group of patients, due to the burn disease itself
Results From the G.I. tract there were no episodes of diarrhoea. TEN was very well tolerated from the very first hours of administration since there was no evidence of paralytic ileus in any patient. All side effects from the upper G.I. tract were observed in one patient in group B. Due to persistent vomiting, t c quantity and rate of administration was initially modified and then temporarily discontinued. Bowel distension was observed in one patient in group A and this was relieved by modifying the quantity (Tab. 5).
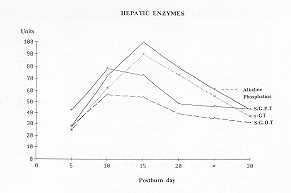
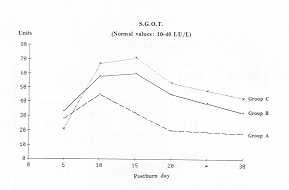
All hepatic enzymes showed an increase
between the 7th and 17th post-burn day and they all returned to normal levels after the
20th post-burn day, although there was no modification in the administration of early TEN
(Fig. 1).
In group A all five patients, with an average age of 35.2 yrs, survived. The duration of TEN averaged 22.6 days (Tab. 6). In group B the four patients, with an average age of 31 yrs, survived their burn injuries. The mean duration of TEN was 62.3 days, since in one patient it was discontinued because of very poor cooperation (Tab. 7). In group C four patients were included, with an average age of 68.7 yrs. Two out of the four patients died on the 7th and the 10th post-burn day and the duration of TEN for the survivors was 52 days (Tab. 8).
The overall morbidity was 15.4%, including
one patient with pulmonary infection in group A, and one patient with wound sepsis in
group C.
Discussion It is an established practice, in most
bum units, to commence TEN after ihe 3rd post-bum day, due to the fear of post-burn
paralytic ilcus. This delay in the initiation of TEN eliminates its advantages of blocking
the hypermetabolic response at a lower ratio.
All side eftects were mild and were
quickly faced by modifying the dosage or the administration rate of the semielemental
diet. High compliance rates were achieved for Keal and proteins administered.
In conclusion, this study makes it clear that TEN is well tolerated, irrespective of the time of its initiation.
RÉSUMÉ. La nutrition entérique totale (NET) à la suite des lésions thermiques représente une nouvelle technique clinique utilisée depuis seulement deux ans, et sa validité suscite encore du scepticisme. Il est l'opinion génerale que la NET doit commencer seulement le troisième jour après la brûlure à cause du danger de l'iléus paralytique. Les Auteurs ont étudié la tolérance de la NET précoce à la suite des lésions thermiques et ses effets collatéraux cliniques et biochimiques. Chez trois groupes de patients (n. 13, TBSA 20-75%) la NET a été commencée respectivement dans les premières heures après la brûlure, le premier jour après la brûlure, et entre le deuxième et le cinquième jour après la brûlure. Les résultats indiquent que la NET a été tolérée en manière suffisante, sans importants effets collatéraux gastriques ou intestinaux ni effets collatéraux irréversibles sur le tissu hépatique. Tous les effets collatéraux ont été légers et faciles à résoudre. La morbidité était basse à cause de l'amélioration des conditions générales des patients, de l'absence d'hémorragie du tube gastro-intestinal et de la réduction de la septicémie. Aussi la mortalité était réduite en manière significative. On peut donc conclure que la NET est une technique bien tolérée, indépendamment du moment de son commencement. BIBLIOGRAPHY
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||