Annals of the MBC - vol. 3 - n' 3 -
September 1990
THE SURGICAL
TREATMENT OF BURNS: SKIN SUBSTITUTES
Magliacani G.
Dipartimento di Chirurgia Plastica e Centro Ustioni,
Centro Traumatologico di Torino, Italia
SUMMARY. An ample survey is
made of the various surgical techniques that may be used in the treatment of bums. The
ditlerent types of skin grafts are described, and the causes of success or failure to take
are considered. A detailed study is made of the various types of skin substitutes, which
may be synthetic (hydrocolloid, polyurethane, polypeptide), biological (fresh and frozen
allogenic skin, fresh and frozen amnion, bovine collagen, animal skin, homologous
keratinocyte culture) or biosynthetic (combination of collagen and a silicone membrane).
The techniques of skin culture are described, thanks to which 2 or 3 CM2 of full-thickness
biopsy can be expanded into 2 M2 of autologous epithelium. Cultured keratinocytes are
therefore especially useful in patients with extensive bums. A comparison is made of the
different surgical strategies to be followed in limited extension burns ( < 25% TBSA)
and extensive bums.
Injured tissue following thermal trauma
constitutes a notable source of toxic substances that, once reabsorbed, have a negative
influence on pathological phenomena both locally and generally in the bum disease.
This is further aggravated by the peculiarity of the damage to the tissue which presents a
central area of necrosis, without vascularity, surrounded by a stasis zone in which cell
metabolism is slowed down, creating favourable conditions for bacterial contamination in
the wounds.
The bacterial colonization is responsible both for the deepening of the wounds by lysis of
the surrounding healthy tissue, and for infection, the most feared and serious
complication in the bum patient.
The excision of necrotic tissue and the covering of excised areas give local advantages,
by eliminating lactic-acid-rich necrotic tissues. These tissues influence collagen
synthesis, by reducing the phlogosis soluble mediators that act on the microcirculation
and the impermeability of the blood vessels, increasing antibacterial defence from
external contamination.
General advantages are also obtained by removing toxic materials with protease activity,
reducing hydro-electrolytic, protein and heat loss, decreasing the risk of sepsis and
shortening the length of hospital stay.
Surgical intervention is therefore a must in the treatment of the acute phase of the burn
patient.
The aim of surgical treatment is to transform the bum wound (avascular lesion) into a
uniformly bleeding non-contaminated surgical wound, at the same time avoiding the process
of eschar demarcation due to granulation tissue, which is the cause of hypertrophic scars.
Surgical treatment, when possible, must be performed between the third and tenth day
post-bum.
The techniques used are:
- tangential excision (Fig. 1), which consists in the
progressive excision of thin slices of necrotic tissue until healthy tissue is reached;
- necrectomy (Fig. 2), which is the excision, en bloc, of the
whole necrotic area;
- dermoabrasion (Fig. 3), i.e. the removal of cellular debris
and dried secretions by means of an abrasive wheel.
 |
 |
| Fig. 1 |
Fig. 2 |
 |
 |
| Fig. 3 |
Fig. 4 |
|
Sometimes a combination of all three may
be used.
The areas prepared in this way must then be covered with free skin grafts to obtain
definitive healing.
Free skin grafts refer to the moving of skin from one part of the body to another,
severing the skin's local blood supply.
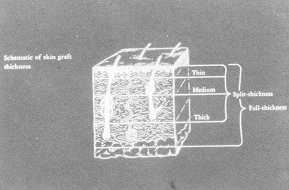
Skin grafts are of two types (Fig. 4): full-thickness grafts and split-thickness grafts.
The full-thickness graft refers to the transfer of the epidermis and complete dermis from
their original site. This graft more closely approximates normal recipient skin in colour,
texture, hair growth and failure to contract. Usually it is smaller in area than the
split-thickness graft, as the donor site is usually sutured for closure.
The split-thickness graft refers to the transfer of the epidermis and a portion of the
dermis from the site of origin. It will less closely resemble normal skin and contracts
more than the full-thickness skin graft.
This division varies in thickness from 0.010 to 0.025 inches in the normal individual.
The donor area refers to the anatomic site from which the graft is harvested, the
recipient site is the bed of tissue on which the free skin graft is placed.
The recipient bed must be vascular, in a qualitative sense, and should be vascular enough
to produce granulation tissue spontaneously.
Exposed bone, cartilage, tendon and nerve are usually unfavourable sites for graft
survival, but periosteum, perichondrium, peritenon and perineurium all have sufficient
blood supply to promote graft survival.
The recipient site, besides being vascular, must also be free of pathogens.
Normal bacterial flora, especially in a noncompromised host, will not interfere with graft
survival, but even a small concentration of pathogens can cause free graft failure.
The most common pathogens causing graft failure are coagulase-positive Staphylococcus,
Pseudomonas and beta-haemolytic Streptococcus.
Grafts may be divided into autologous, allogenic and xenogenic.
In the autograft the donor and the recipient are the same person, in the allograft the
recipient is different from the donor (live or cadaver) and in the xenograft the graft is
taken from a different species (bovine or swine).
The first choice technique is the use of an autograft, as only the autograft takes
permanently, healing as in surgical repair, by means of direct contact of the two cut
surfaces.
Graft take, the process that must occur for free skin autograft to survive, depends on the
ability of skin to have its blood supply severed and then reformed without direct
reattachment.
There are three major factors in the success of skin grafts.
The first is a vascular recipient bed free of pathogenic bacteria.
The second is the vascularity of the graft itself. Thin split-thickness grafts are more
vascular on their undersurface than thick split-thickness or thick full-thickness grafts.
This difference in vascularity is due to the fact that thin grafts have a very rich
capillary network. The survival of a thin split-thickness skin graft is therefore higher
than that of a thicker one.
The third factor affecting graft take is the maintenance of contact between the skin graft
and the recipient bed.
Proper tension must be placed on the graft and meticulous haemostasis prior to placement
is critical, as the presence of secretion or haematoma prevents contact between graft and
recipient site, impeding take.
The graft take occurs because of plasmatic imbibition, the initial fibrin glue that
attaches the graft to the recipient bed,and, subsequently, of inosculation of blood
vessels, the growth of the vascular buds into and through the fibrin network, binding the
skin to the recipient site. Inosculation of blood vessels usually begins around 48 hours
after the graft is placed.
The principal causes of graft take failure are infection, bleeding and insufficient
pressure on the recipient site.
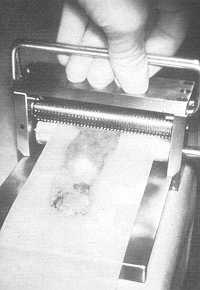
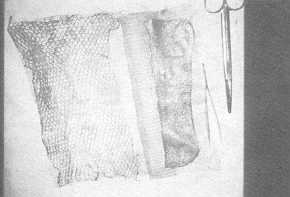
In burn wounds, thin split-thickness grafts are usually employed, because of their easier
take and the more rapid healing of the donor areas.
Mesh-grafts are often used to increase the available skin (Figs. 5-9).
 |
 |
| Fig. 5 |
Fig. 6 |
 |
 |
| Fig. 7 |
Fig. 8 |
 |
Fig. 9 |
|
In extensive lesions, when a large enough
appropriate donor site is not available to cover the wounds or when there is doubt that
the recipient surface is viable, skin substitutes may be used.
Skin substitute
Skin substitutes may be divided into
synthetic, biological and biosynthetic. They have been advocated as a means of temporary
wound closure until spontaneous or surgical healing can occur.
Their characteristics must include protection from external contamination, reduction of
water, electrolyte and heat loss, pain relief and relative case of application.
At a later date, if necessary, the treated areas or the newly formed granulation tissue
may be covered.
Synthetic dressings
Superficial partial-thickness bums may be
treated by a variety of methods.
Various dressing materials have been proposed, all with the aim of facilitating
spontaneous burn,' wound healing.
Although they have no analogy with live tissue, these materials must be neutral, and have
such characteristics as adherence and flexibility for an easy dressing in difficult areas
(such as the genitalia and the face), protection from external contamination, water vapour
transmission, fluid escape without causing wound, desiccation, non-inclusion in the wound
and low cost.
They must also decrease the healing time, because this improves the quality of healing.
Many of the materials available today not only have these characteristics but also respond
to other needs emerging from more recent studies, i.e. they maintain a humid environment
that inhibits the formation of crusts, and thus favours spontaneous healing.
Such new materials adhere to the surrounding tissues and not the lesion itself, thus
forming an impermeable isolated environment which is ideal for healing.
Dressing with traditional paraffin gauzes has been shown to have a purely protective
mechanical effect on the wound healing.
These gauzes do not however prevent either the drying of the lesion or crust formation,
both of which cause considerable pain in movement.
Our Centre uses hydrocolloid dressings, polyurethane films and membranes prepared from a
synthetic polypeptide.
Hydrocollold dressings are useful in many clinical situations, but the most correct
indication is their use on split-thickness burns (Figs. 10- 15) and donor sites (Figs.
16-18) in which an optimal spontaneous healing environment is created, usually in 7 to 15
days.
 |
 |
| Fig. 10 |
Fig. 11 |
 |
 |
| Fig. 12 |
Fig. 13 |
 |
 |
| Fig. 14 |
Fig. 15 |
|
They are painless, easy to apply but must
be placed on sterile surfaces, like all synthetic dressings.
 |
 |
| Fig. 16 |
Fig. 17 |
 |
 |
| Fig. 18 |
Fig. 19 |
 |
 |
| Fig. 20 |
Fig. 21 |
|
On contact with the lesion the
hydrocollold surface interacts with secretions, forming an absorbing gel. It also has a
pressure eftect.
Dressing is performed every 1-2 days at the beginning, after irrigation with a saline
solution and drying the edges to obtain optimal adhesion. It is then left in position
until healing is obtained.
The need to change the dressing more frequently at the beginning is due to the fact that
the hydrocolloidal layer liquefies in contact with the humid lesion, forming a liquid that
oozes out of the dressing.
The absence of side effects, the ease of use and the good level of tolerability allow us
to pass a favourable judgement on this type of dressing.
The polyurethane and polypeptide films are thin synthetic membranes which, with varying
porosities, favour a barrier effect by conserving their impermeability to liquids and
environmental oxygen. These can be used only in wounds of limited size as they adhere
exclusively to healthy skin.
Biological materials
Among the biological materials used in
burn wound covering we must not forget fresh and frozen allogenic skin, fresh and frozen
amnion, bovine collagen, animal skin and homologous keratinocyte culture.
Allogenic cadaver skin is the ideal biological coverage, because of its histological
similarity to the biological tissue to be replaced.
The possibility of freezing and stocking for many months makes this type of graft an
excellent and readily available skin substitute.
Skin allograft is able to take in the same way as an autograft,' favouring the formation
of granulation tissue, on to which the definitive graft may be placed.
When numerous allografts have to be used in the same patient, it is advisable to change
donors, in order to avoid sensibilization, which would lead to a shorter survival of the
graft.
Skin allograft, to a lesser extent than skin autograft, limits bacterial colonization by
means of an antibacterial action on the recipient bed.
Nevertheless, its biological individuality, immunologically speaking, generally provokes a
rejection reaction.
The use of histocompatible or irradiated grafts and/or the administration of
immunosuppressants allows the graft to remain for several weeks, easing the many problems
involved in coverage.
Recently some methods have been proposed enhancing the results obtained by allografts: the
Chinese technique which consists in autogenic skin islets in intermingled meshed skin
allograft; the wide-meshed autograft covered by meshed dermo-epidermal allograft or
cultured epithelium allograft; the split-thickness allograft on to which, after the
removal of the epithelium by dermoabrasion, the autologous cultured epithelium is placed.
By this process the three-dimensional texture of the allodermis is grossly preserved and
can be demonstrated even after years.
This apparent acceptance of allogenic tissue, which diverges from current knowledge about
the immunological process of graft rejection, remains to be explained.
The skin graft must be taken from donors who are negative for syphilis, hepatitis B virus
(HBV) and human immunodeficiency virus (HIV) and are non-carriers of systemic or chronic
infectious diseases.
The removal of skin from . cadavers may sometimes be conditioned or made impossible by
current legislation.
Many researchers have used amniotic membranes in various clinical situations including
burns, as they are both easy to obtain and use and inexpensive.
Amnion obtained from healthy mothers must be washed and conserved in an appropriate liquid
(Me Coy modified) at 4 'C for a maximum of 3 weeks before use.
The amniotic layer is separated from the chorion. If a split-thickness lesion is to be
covered, the amniotic layer is used, but if a full-thickness lesion is involved the
chorial layer is employed, as it has bacteriostatic properties similar to that of skin
allografts which seem to regulate the procollagen synthesis in the exposed area and
stimulate better growth of the granulation tissue that is to be covered, at a later date,
by autografts (Figs 19-23).
 |
 |
| Fig. 22 |
Fig. 23 |
|
Amnion permits optimal adherence to the
recipient bed, thanks to its particular adaptability, and the process of
re-epithelialization can be verified from the very beginning, because of its transparency.
For this reason amnion is preferable to other biological dressings.
No rejection phenomena have so far been reported, and there are no data available as to
the antigenic activity of amnion.
On the other hand we cannot speak of "take" in the real sense of the word, as
there is no vascular connection between the recipient bed and the applied membrane.
In our experience, the best results can be obtained by early application on thin
split-thickness wounds, when treating facial split-thickness burns after dermoabrasion,
and in the dressings of donor sites.
Although the above cases have spontaneous re-epithelialization, the type of dressing
chosen has an important effect both on healing time and on the quality of the healing
itself, as does the sterility or low contamination of the recipient bed.
An important element favouring this result is the limited number of dressings necessary,
which reduces the probability of exogenous infections.
In our experience with amnion, we did not note the presence of the ' bacteriostatic effect
which is present in allogenic skin grafts.
This may be due to the more frequent dressings carried out by other researchers.
When amnion was used as temporary coverage after full-thickness burn excision, its
biological value was found to be inferior to that of skin allografts. Nevertheless, its
high tolerability and its ability to reduce pain prove it to be a useful material as a
biological dressing in the burn patient.
Animal skin has a lower biological level than the others, having no affinity with the
recipient bed, no ability to stimulate the formation of granulation tissue and no control
over infection. It can however be used as an alternative form of coverage.
Once it was used fresh but nowadays it is distributed, at high cost, preserved and
impregnated with silver sulphadiazine, for use as a permanently available antibacterial
dressing.
Bovine collagen can used in the treatment of small lesions; it is gradually reabsorbed by
an enzymatic action on the part of substances present in the lesion, and has only a
protective role.
Among the various biological materials, allogenic epithelial culture must be mentioned.
This will be discussed below in greater detail.
There is also another form of biological dressing that has recently been proposed, this
time of vegetable origin. This is a bandage of boiled potato peelings.
The cleaned peels are collected from hospital kitchens, stuck with starch paste to roller
bandages, packed in plastic bags and sterilized.
This bandage considerably simplifies the dressing of burn wounds and may make this form of
dressing more useful and acceptable to burn units developing countries.
Biosynthetic materials
These are formed by a layer of
collagen adherent to a silicone membrane. They have been found very useful when temporary
coverage of surgically exposed areas is necessary, until definitive coverage may be
carried out.
Some authors consider them to be first choice treatment for superficial partial skin
thickness burn wounds.
Although the dressing has a high cost, it is changed less frequently than other topical
materials. Out-patient care is therefore possible, resulting in a decrease both in the
length of hospital stay and the ultimate cost of burn care.
Very deep wounds will not allow dressing adherence, nor will it occur if the wound has a
high bacterial count.
The presence of many varied materials of different utility for the coverage of burn
lesions necessitates the preparation of indication indexes in order that they may be used
optimally.
As exposure of the burn implies a high risk of necrosis in deep tissues, the different
nature of the various dressings means that a careful choice of the material to be used
must be made.
On the whole the use of biological dressings in epidermal burns gives the best results, if
applied on a sterile recipient bed, because of their ability to stimulate a quicker
spontaneous healing.
However synthetic materials are often preferred to biological ones, due to the fact that
they are more easily available.
In the treatment of dermal burns, skin allograft, cultured allogenic epithelium and amnion
give the best results.
This is because they have a positive effect on the processes involved in spontaneous
healing and carry out a bacteriostatic activity, which maintains a favourable environment
on the interface between dressing and lesion.
In the presence of full-thickness burns, when immediate permanent coverage is not possible
after surgical excision, the area may be temporarily covered with cadaver skin, which may
later be replaced by skin autograft.
Alternatively, even if less satisfactory, amniotic membrane may be used for this function.
The use of animal skin or synthetic materials is not indicated.
Biosynthetic material has proved useful as it is able to protect the recipient bed from
deepening and bacterial contamination.
Although this is a less valid biological solution with a high cost, this material is
always available when others are not. In the treatment of donor sites, all the above
materials may be used, with the same results in terms of time and quality of healing.
Availability and cost should therefore be taken into account when the choice of dressing
in made.
Skin culture
Cultured human epithelium, the use of
which is not easy, has recently been introduced into burns therapy.
With only 2 or 3 CM2 of full-thickness biopsy 2 M2 of autologous epithelium may be
obtained.
In the past many researchers were attracted by the idea of finding a solution in vitro to
the covering of extensive areas of destroyed skin.
A solution was found when Green obtained a culture of keratinocytes.
After its introduction and successful clinical application its more frequent use was
encouraged.
The skin biopsy (Fig. 24) must be taken as soon as possible, preferably on admission, as
the trauma involved is insignificant and there is no risk of bacterial contamination of
the healthy skin in the first few days.
The ideal donor sites are the mastoidal area, the arm-pit region, the groin and, in the
male patient, the prepuce and scrotum skin at full thickness.
The skin, once in the laboratory, is minced and trypsinized to separate the epithelial
layer from the dermis and the resulting cells are inoculated in flasks containing lethally
irradiated mouse fibroblasts (Fig. 25).
Small non -differentiated basal cells form colonies that grow at the periphery, and the
cultures become confluent in 9-15 days.
Primary cultures are passaged in secondary cultures and, within two weeks, the confluent
epithelium formed by thin epithelial layers made up of 7 or 8 cell strata is detached from
the surface vessels with neutral protease (Dispase 11), washed in serum-free medium and
placed basal side up on sterile vaseline gauze cut into 50 CM2 pieces (Fig. 26).
The grafts can be transferred to the burns unit (Fig. 27) if placed in Petri dishes which
are put into a plexiglas box equilibrated with IMO C02-
 |
 |
| Fig. 24 |
Fig. 25 |
 |
 |
| Fig. 26 |
Fig. 27 |
|
The keratinocyte layers may then be used
immediately (Fig. 28) to cover the areas of destroyed skin, frozen until needed, or used
in new cultures to increase the quantity of available material.
There is an inverse correlation between the patient's age and the growth rate of cells in
culture, which is quicker in children and slower in adults over 60.
This depends on a lower colony-forming efficiency of keratinocytes isolated from older
donors, because the number of holoclones, which have the highest growth potential,
decreases with natural aging. The use of cultured keratinocytes must be limited to
extensive burns, with well-defined clinical situations, i.e. grafts on deep burns after
excision at the muscular fascia, after necrectomy and the use of temporary coverage with
bio-compatible materials, in the coverage of donor sites and also in the protection of
split-thickness burns. Today this is the only method which may be employed in patients
with burn areas so extensive as to exclude the use of more traditional methods.
Histological studies have shown that the transplanted epithelium thickens within a few
weeks, has the same layers as those present in normal skin, has a basement membrane zone
and contains well-differentiated and physiologically placed melanocytes, but there are no
epithelial crests or dermal papillae. The underlying dermis has a modest inflammatory
response, similar to that seen in areas healed by spontaneous reepithelialization or after
coverage with traditional autografts.
Biopsies performed in the first three weeks after graft-take and examined under electron
microscopy showed the presence of Langerhans cells from the second week. These were also
visible later under optical microscopy. The most difficult problem in the use of cultured
autograft is that of the preparation and the conservation of a suitable recipient bed. In
fact most researchers have attributed failures to infection in the recipient bed, which
leads to a bacterial lysis of the transplanted epithelial layers. The most successful
method is that of early excision of the burn tissue as far as the muscular fascia, as
cultured keratinocytes adhere best if placed directly on the fascia, well on deep dermis
and badly if in contact with subcutaneous fat.
Temporary coverage is then effected on the exposed areas with cadaver skin grafts from a
tissue bank. In this way the risk of wound infection is avoided, giving an optimal if
temporary coverage, with the possibility of cultured epithelium skin grafts on a non
-contaminated recipient bed, after 3 or 4 weeks. The lack of cadaver skin banks in many
countries (including Italy) necessitates the use of other methods which involve more
difficult processes of maintaining a non -contaminated recipient bed suitable for skin
graft, in the time interval between skin biopsy and the supply of cultured keratinocytes.
In our opinion there is no easy solution to the problem, as ammon gives an excellent
temporary coverage for I or 2 weeks, but does not ensure sterility of the recipient bed
until the culture is available, in the case of early excision of necrotic
tissues.Bacterial flora is controlled but not suppressed with topical treatment and the
results obtained using cutaneous substitutes of various nature, although encouraging, are
far from fully satisfying.
However, results obtained in our early experiences with Biobrane seem to be positive, and
agree with those of other authors.
Lastly, the fragility of the graft presented another difficulty when autologous
keratinocytes were used, as during dressing the graft may be inadvertently removed from
the recipient site so that its take capacity is lost.
The grafts were sutured on the recipient bed, covered with sterile gauze and modest
pressure was applied.
A few days days later (3 to 5), the dressing was removed (Fig. 29) and the skin graft was
left exposed to environmental air.
The Turin Burns Centre began clinical experiments in 1986, using cultured autografts on
burns in over 50 patients (Figs. 30-33).
 |
 |
| Fig. 28 |
Fig. 29 |
 |
 |
| Fig. 30 |
Fig. 31 |
 |
 |
| Fig. 32 |
Fig. 33 |
|
This technique proved to be useful in many
patients, in particular in those cases with a more severe prognosis, in whom it was indeed
a life-saving procedure, even if the take percentage did not exceed on average 35% of the
covered area.
Its further use as allograft may be that of the treatment of deep second-degree and
limited full-thickness burns to obtain spontaneous healing (Figs. 34-37).
 |
 |
| Fig. 34 |
Fig. 35 |
 |
 |
| Fig. 36 |
Fig. 37 |
|
This technique has given good results in
older patients especially when cultured allografts were obtained from young donors.
These grafts were applied to most donor sites and good quality healing was obtained.
This application can be extremely useful in reducing exposed areas in patients with
infected wounds and in preventing the formation of hypertrophic scars in donor sites.
Results have been less satisfactory in the temporary covering with fresh or frozen
cultured allografts of excised areas which cannot be immediately covered with autografts
either due to unavailability or to dubious viability of the recipient bed.
Cultured allografts have a reduced antibacterial activity and offer poor mechanical
resistance.
Together with the clinical use of allografts studies have been performed which, although
giving contrasting results, are worth noting.
Early observations of the permanent take of epidermal allografts have been followed by
proof that such a take is not possible.
The apparent non-rejection may be explained by the survival of transplanted cells without
a real biological take.
The cultured keratinocytes present on the recipient bed are able to produce important
growth factors, such as EGF and Transforming Growth Factor, which modulate their gradual
substitution with autologous cells.
Apart from any scientific considerations, cultured keratinocytes are a reality and must be
regarded as a therapeutic means for definitive or temporary coverage of burn wounds.
Their recent introduction into burn therapy leads us to make some considerations.
Human cultured keratinocytes can be successfully used as permanent wound coverage after
bum excision, and their use in burn wound coverage may constitute an additional method to
limit mortality in burn patients.
However it is first of all very important to coordinate the culture staging and the
surgical schedule so that the culture will be in an optimal condition when the recipient
site is ready to be grafted.
Therefore it is important to calculate the time lapse between biopsy and the grafting of
confluent secondary culture.
A freezing protocol was set up for stable grafts to minimize the timing problems and to
facilitate long-distance transportation, allowing us to have epidermal sheets at our
disposal whenever necessary, independently of cell culture timing.
Studies on cultured epithelium have led to the following considerations, in part
previously mentioned:
- There is an inverse correlation between the patients' age
and the time lapse between biopsy and transplantation.
- The different growth potential and life time of cultured
keratinocytes may also be one of the factors why the take is better in young patients.
- Early granulation tissue appears to be a much better
receiving bed than does chronic granulating tissue.
- Muscular fascia has been reported to be the ideal receiving
bed but especially in young patients the problems of subsequent scar retraction of the
grafted area is highly increased.
- Cultured keratinocytes may be a life-saving factor in bum
patients with over 50% of the body surface damaged with full-thickness burns.
- At present cultured epithelium is too expensive a method to
be used in patients under the 50% limit.
The use of cultured allogenic
keratinocytes must still be considered experimental as, at the present stage, it is
impossible to define its behaviour with regard to the recipient bed and therefore its real
therapeutic capacity, above all if the high cost is taken into consideration.
Our observations, if compared to those found in the literature, allow us to express
positive evaluations on the results obtained to date, even if there are some difticulties
to be faced in clinical applications on a large scale.
Although the present keratinocyte culture does not yet represent the ideal skin
substitute, it seems today to be the only method of resolving critical situations stemming
from extensive bums.
Conclusions
To conclude this review of skin
replacement, we wish to emphasize how essential surgical treatment is in deep and
extensive burns and how the degree of gravity of the patient requires its own careful
schedule and execution.
The strategy should differ if less or more than 25% TBSA is involved, because of the
different systemic involvement and the various organizational problems.
In the case of limited extension burns, surgical intervention should be programmed
within the first week, for diagnostic and therapeutic ends.
In this way, the depth of the lesion may be estimated more accurately with surgical
intervention before the onset of septic factors that complicate the clinical picture.
Surgical toilet of the lesions and excision of necrotic areas or dermoabrasion of all
devitalized fissues, carried out in the operating theatre, should be followed in the case
of full-thickness burns by autologous skin grafts which will lead to quicker healing.
Mesh-grafts are recommended except when the face and hands are involved.
After surgical toilet, split-thickness burns may be covered by amnion or cultured
allografts.
Spontaneous re-epithelialization was observed when using this technique, particularly in
younger patients.
When more than 25% of the body area is involved the strategy is more complex.
Whenever possible, skin biopsy should be taken on admission, in order that skin culture
may begin.
On surgical intervention no more than 15-20% of BSA necrotic tissues should be removed at
one time, giving priority as always to the face and hands.
In the presence of a viable recipient bed, traditional skin grafts are used if available.
If not, cultured grafts are employed.
In doubt, before definitive coverage is effected, various alternative materials may be
used: cadaver skin, amnion, alloplastic cultured epithelium (fresh or frozen), synthetic
skin substitute or, when such materials are not available, Vaseline gauze and
antibacterial agents such as polyvinyl pyrrolidone, iodine, chlorhexidine and others.
The outcome of burns treatment will be further improved only when optimal operating times
and clear technical criteria have been established.
The concepts expressed here, which represent a number of today's trends, constitute
indications in this direction.
RÉSUMÉ. Après avoir exposé amplement les
différentes techniques chirurgicales utilisées dans le traitement des brûlures,
l'Auteur décrit les divers types de greffes cutanées et considère les causes du succès
ou de l'insuccès de la prise. Il continue avec une analyse détaillée des divers types
de substitut cutané, qui peuvent être synthétiques (hydrocolloïde, polyuréthane,
polypeptide), biologiques (peau allogénique fraîche ou congelée, amnios frais ou
congelé, collagène bovin, peau d'animal, culture de kératinocytes allogéniques) ou
biosynthétiques (association de collagène et membrane de silicone). Il décrit les
techniques de la culture de la peau, qui permettent d'obtenir 2 M2 d'épithélium avec
seulement 2 ou 3 CM2 de biopsie à toute épaisseur. Les kératinocytes cultivés sont en
conséquence particulièrement utiles chez les patients avec brûlures étendues. En
conclusion, il y a une comparaison entre les diverses stratégies chirurgicales qu'il faut
adopter pour les brûlures moins étendues ( < 25% TBSA) et les brûlures éténdues.
|