Annals of the MBC - vol. 3 - n' 3 -
September 1990
AN EPIDEMIOLOGIC
STUDY OF BURNS
Benito Ruiz J., Navarro Monzonis A., Baena Montilla P.
Department of Plastic Surgery and Burn Centre Hospital La
Fe, Valencia, Spain
SUMMARY.
We report a retrospective epidemiological study based on 710 charts of patients admitted
to our Burn Centre between 1985 and 1988. During this period we assisted 9794 people at
our Casualty Centre. The average age of the patients was 24 yrs and 66% were males. Burns
were much more frequent in children < 10 yrs, especially due to scalding by hot water.
Nearly 47% were children under 15 years old. The two leading causes were scalding and
flames. Other significant causes were gunpowder and electricity. Contact burns, fire and
chemicals were less frequent. Massive burns were due to flames and gunpowder. The deepest
lesions were produced by electricity and contact burns. Regarding the place where the
accident happened, burns occurring in the home were due to scalding and fire. Accidents
outdoors were produced by improper use of gunpowder and by electricity (high voltage).
Work-related accidents occurred mainly to chemists and electricians. Males outnumbered
women regarding street and work-related accidents (p <0.000001). The face and neck were
most commonly afTected when the cause was flames and chemicals, the trunk and upper limbs
in the case of scalds and flames, the lower limbs with flames and hot contact, and the
hand and wrists with electrical and gunpowder injuries. Gunpowder and scalds were involved
in genitalia burns.
Introduction
Burns are one of the most frequent
injuries treated in a Casualties Service, and they carry an important medical, social and
economical cost. Medical management of these injuries has improved considerably in recent
years and the survival of even very severel~ burned patients is being achieved.
Nonetheless the best way to cope with the problem is to prevent it. A proper burn
prevention programme must be based on previous studies about causes, population groups
affected and where the injury takes place, etc. These data are provided by epidemiologic
studies from the Burn Centres.
The aim of this work was to identify the epidemiologic features of the burn injury in our
community in order to accomplish a new programme of prevention.
Material and methods
We have reviewed 710 charts of
patients who were admitted to our hospital from December 1984 to December 1988. During
this period we assisted 9794 patients at our Casualties Service. 9084 out of them were
managed as out-patients, which makes an admission rate of 7.25%.
Data were stored and subsequently analysed on a database programme.
Results
Age
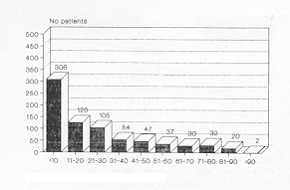
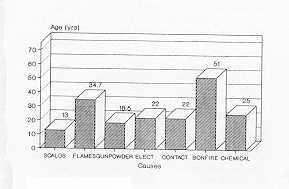
The average age was 23.84 +/- 24.06 years. Fig. 1 shows
the number of patients by age groups. We should point out that 333 patients (46.9%) were
children under 15 years old.
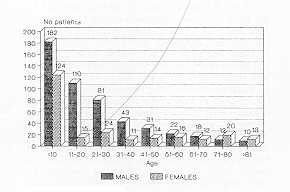
Sex
469 out of the 7 10 patients were male
(66%). This predominance occurs for all ages (Fig. 2), except for elderly patients (
>70 yrs), in which case women were slightly more numerous than men. This is probably
due to the greater female population at this age.
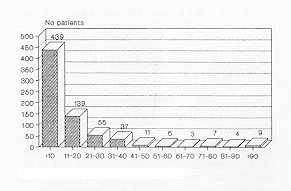
Burn size
The average burn size was about 14% (14.04
+/17 ' 76%). Fig. 3 depicts the distribution of the patients regarding burned body
surface. 113 out of the whole total (15.9%) sustained extensive burns ( >30% TBS), and
61.8% had minor burns ( <10% TBS).
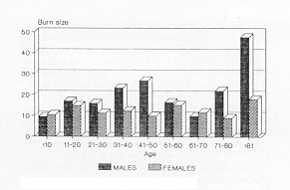
The mean burn extent was larger in general terms in the male population (Fig. 4), except
for children under 10 yrs and women between 61 and 70 yrs, but the difference was not
statistically significant.
There were minor differences regarding burn size and cause of injury. Nevertheless, women
sustained the largest burns by gunpowder, fires and chemicals (Fig. 5).
 |
 |
| Fig. 1 Distribution
of patients by age |
Fig. 2 Distribution
by sex |
 |
 |
| Fig. 3 Distribution
of patients by bum size |
Fig. 4 Distribution
of burn size by sex and age |
 |
 |
| Fig. 5 Average
bum size by sex and cause |
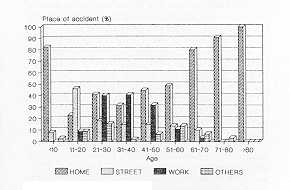
Fig. 6 Age/Accident
Relationship |
|
Type of accident
We have distinguished three main groups
depending on the place where the injury happened: home, street and work-place. These three
groups comprise 91.9% of the burned population. The rest (8. 1%) includes traffic
accidents, sport-related injuries, self-induced and criminal burns (aggressions), and
others (e.g. sunburn).
The most frequent site of the burn injury was the home (43 5/7 10, followed by the street
(119) and the work-place (99). The distribution of the burned population by agd and type
of accident is displayed in Fig. 6. Accidents in the home were especially frequent at
extreme ages. 82.67% (253/306) of patients under 10 yrs, and 89.28% (75/84) of patients
above 60 yrs sustained bums at home. Injuries as a result of playing in the street were
frequent in patients between 11 and 20 years old (46%, 58/126). Patients from 21 to 60 yrs
were more often injured at work, accounting for 40.25% of the accidents at this age
(64/159).
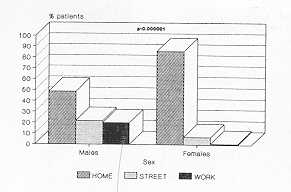
Regarding sex, injuries produced in the home affected women more frequently than men
(85.9% vs 48.6%), whereas street- (7% vs 21.7%) and work-related accidents (1% vs 20%)
were predominant in men (p < 0.00000 1) (Fig. 7).
Causes
The different causes of the burn injury
have been broken down as follows: scalds, flames, gunpowder, electrical, hot contact,
fire, chemicals and others. Burns by fire refer to those produced mainly by live coals or
braziers, but also sometimes by lighters, candles, the burners of cookers and heaters,
depending on the personal view of the physician on call.
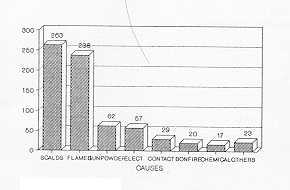
Scalds (263/710) and flames (263/710) were the most frequent causes involved in the burn
injury (Fig. 8).
The average age varied in relation to the cause (Fig. 9). Fire affected people in general
(mean 51.5 yrs), whereas gunpowder, electricity, hot contact and chemicals affected young
adults. Children are commonly burned by hot liquids (scalding).
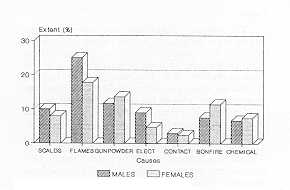
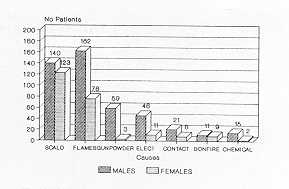
Males were in general more affected regardless of the cause of injury. The difference
between the sexes was greater when the burn was provoked by gunpowder, electricity and
chemicals (Fig. 10).
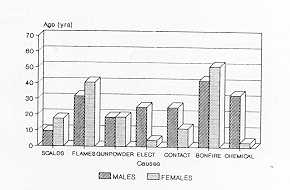
We have observed that the average age in females was higher for all causes except
work-related burns (electrical, hot contact and chemicals) (Fig. 11).
 |
 |
| Fig. 7 Sex/Accident
Relationship |
Fig. 8 Frequency
of causes |
 |
 |
| Fig. 9 Average
age by causes |
Fig. 10 Distribution
by sex and causes |
 |
 |
| Fig. 11 Average
age by sex and cause |
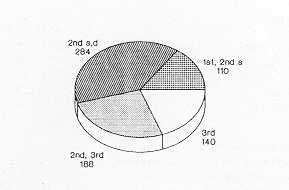
Fig. 12
Bum depth |
|
Table 1 shows the main causes of the bum
injury in relation to age. Children were most commonly affected by scalding (64%), and
flames were the most frequent cause for the rest of patients, being the exclusive cause of
the burn injury in patients above 80 years. Gunpowder (fireworks) was an important cause
in teenagers. Electrical and chemical burns corresponded to working ages (10.6% and
4.76%). Fire and hot contact afTected aging patients (61-80 yrs).
Regarding the place where the accident happened, we found that scalds, flames, hot contact
and bonfire were mainly domestic (94%, 52%, 69%, and 85% respectively); gunpowder burns
were street accidents (83,9%) and electrical and chemical injuries happened at work sites
(52.6% and 53% respectively) (Table 2).
Bum Depth
Fig. 12 shows the number of patients in
relation to burn depth at admission evaluation. 140 patients had sustained pure
full-thickness burns, and 188 had both partial- and full-thickness burns. Only 15.47% had
sustained minor injuries (simple erythema and/or partial -thickness burns).
Scalding was the commonest cause of first- and second-degree injuries. Flames were
responsible for both second- and third-degree burns. Hot contact and electricity caused
mainly full-thickness burns, whereas gunpowder and chemicals usually provoked deep-dermal
plus full-thickness bums (Table 3).
Location of bums
Table 4 shows the parts of the body
involved by the bum injury on admission, related to the cause. Face and neck burns were
more affected by flames (56.7%) and chemicals (42%); the trunk (chest, abdomen and back)
was involved by scalding (46.7%) and flames (44%), as also the upper limbs (49.8% and 49%
respectively); the wrists and hands were injured by electricity (61.4%) and flames
(41.6%). Burns on the lower limbs were caused by flames (52%) and hot contact (48%)
(exhaust pipes and heaters). Scalding (baths) and gunpowder blasts (from firecrackers and
small rockets kept in the pockets and lighted inadvertently) were the main causes involved
in buttocks and genitalia burns. Injuries to the lips and tongue were exclusively caused
in children by low-voltage electricity. Massive ( >90%T1IS) burns were due to gas and
gunpowder (fireworks industry) explosions.
Length of stay
69.85% of the patients were discharged
from our hospital within two weeks of admission. Nearly 21% were kept as in-patients for
more than five weeks (Table 5). The average burn extent in this group was 23.67%, with
75.85% full-thickness or partial-plus full-thickness burns.
ConiMents
The exact incidence of the burn injury
in our area cannot be estimated from our data from 1984 to 1988, as the national Health
Authority did not establish clearly the population to be covered. In January 1989 a clear
"sectorization" was defined, which will let us estimate our prevalence rate.
Nevertheless, the number of patients assisted at our Casualties Service is very similar
every year and remains stable (about 2000 patients/yr). Most of them have minor injuries
which do not require hospitalization and can be followed on an out-patient basis. Only 7%
required hospital management; 16% presented a burn size larger than 30% (as Clark and
Fromm, 1987).
| CAUSES (%) |
SCALDS |
FLAMES |
GUNPOWDER |
ELECTRICAL |
HOT CONTACT |
BONFIRE |
CHEMICAL |
OTHERS |
| -10 |
64 |
11.4 |
4 |
5.5 |
3.9 |
0.97 |
0.97 |
1.95 |
| 11 -20 |
7 |
38.9 |
24.6 |
6.35 |
3 |
2.4 |
1.5 |
5.5 |
| 21 -30 |
11.4 |
45.7 |
10.5 |
16 |
4.76 |
1.9 |
4.76 |
1.9 |
| 31 -40 |
16.6 |
42.6 |
3.7 |
11 |
5.5 |
0 |
3.7 |
5.5 |
| 41 -50 |
21.3 |
48.9 |
10.6 |
10.6 |
2 |
2 |
2 |
0 |
| 51 -60 |
21.6 |
40.5 |
0 |
8 |
8 |
5.4 |
2.7 |
2.7 |
| 61 -70 |
20 |
56.6 |
0 |
3.3 |
0 |
13 |
3.3 |
3.3 |
| 71 -80 |
28 |
40.6 |
0 |
0 |
9.4 |
9.4 |
3 |
3 |
| +80 |
13.6 |
72.7 |
0 |
0 |
0 |
9 |
0 |
4.5 |
|
| Table 1 Frequency
of causes by age |
|
| LOCATION
CAUSE |
HOME |
STREET |
WORK |
SPORTS |
TRAFFIC |
MEDICAL |
OTHERS |
| SCALDS |
94.3 |
1.5 |
4 |
- |
- |
- |
0.4 |
| FLAMES |
51.7 |
11.3 |
15.5 |
1.7 |
5 |
- |
2.9 |
| GUNPOWDER |
3.2 |
83.9 |
9.6 |
1.6 |
- |
|
1.6 |
| ELECTRIC |
29.8 |
17.5 |
52.6 |
- |
- |
- |
- |
| HOT CONTACT |
69 |
- |
13.8 |
- |
17.3 |
3.5 |
- |
| BONFIRE |
85 |
10 |
5 |
- |
- |
- |
- |
| CHEMICAL |
29.4 |
- |
53 |
- |
- |
17.6 |
- |
|
| Table 2 Cause/place
of accident relationship |
|
A:
first and/or superficial second degree
B: deep dermal and partial-thickness burns
C: second and third degree
D: full-thickness burns
BURN DEPTH
CAUSES |
A |
B |
C |
D |
| SCALDS |
47 |
30 |
30.3 |
19.6 |
| FLAMES |
34.5 |
23 |
43.6 |
28.3 |
| GUNPOWDER |
3.6 |
11 |
10.6 |
10 |
| ELECTRICAL |
4.5 |
10 |
9 |
20 |
| HOT CONTACT |
0.9 |
8.9 |
1.6 |
14.5 |
| BONFIRE |
0.9 |
8.9 |
3.7 |
4.3 |
| CHEMICAL |
5.5 |
8.9 |
1 |
3.6 |
|
| Table 3 Cause/burn
depth correlation |
|
The burns in this, as in other studies
(Silverstein, 1987; Clark and Fromm, 1987), mainly affected young people. The average age
of our patients was about 24 yrs. This is due to the high predominance of children in our
burned population (46.9%), which is in line with other reports (Elberg et al., 1987).
The male population ran twice as much risk of sustaining burns as the female population.
This is because men more frequently handle dangerous substances and devices, both by
playing and by working with them. Not only were there more burned men but they had the
largest burn sizes as well. We found that women older than 60 yrs had larger burns than
males at the same age, which coincides with observations made by Clark and Fromm (1987).
LOCATION
CAUSES |
FACE
NECK |
TRUNK |
UPPER
LIMBS |
HANDS |
LOWER
LIMBS |
BUTTOCKS
GENITALIA |
LIPS
TONGUE |
TOTAL |
| SCALDS |
28.9 |
46.7 |
49.8 |
8.7 |
39 |
13.7 |
- |
- |
| FLAMES |
56.7 |
44 |
49 |
41.6 |
52 |
1.3 |
- |
3.8 |
| GUNPOWDER |
21 |
13 |
21 |
24 |
22.6 |
8 |
- |
3 |
| ELECTRICAL |
31.6 |
22.8 |
33 |
61.4 |
22.8 |
- |
19.3 |
- |
| HOT CONTACT |
13.8 |
13.8 |
20.7 |
24 |
48 |
10 |
- |
- |
| BONFIRE |
30 |
35 |
30 |
15 |
35 |
15 |
- |
- |
| CHEMICAL |
42 |
29 |
35 |
12 |
42 |
6 |
- |
- |
|
| Table 4 Parts
of the body affected by causes |
|
WEEKS
AGE GROUPS |
1 |
2 |
3 |
4 |
5 |
5-8 |
>8 |
| -10 |
178 |
49 |
8 |
11 |
24 |
12 |
5 |
| 11-20 |
57 |
20 |
8 |
3 |
8 |
7 |
10 |
| 21 -30 |
47 |
17 |
12 |
2 |
6 |
9 |
8 |
| 31 -40 |
24 |
9 |
2 |
0 |
5 |
2 |
6 |
| 41-50 |
24 |
6 |
3 |
1 |
4 |
4 |
4 |
| 51 -60 |
15 |
2 |
5 |
3 |
0 |
2 |
5 |
| 61 -70 |
15 |
2 |
3 |
0 |
1 |
2 |
7 |
| 71 -80 |
13 |
2 |
1 |
1 |
2 |
5 |
6 |
| +80 |
15 |
1 |
0 |
2 |
2 |
2 |
1 |
| TOTAL |
388 |
108 |
42 |
23 |
52 |
45 |
52 |
| % (N = 710) |
54.65 |
15.2 |
5.9 |
3.24 |
7.3 |
6.34 |
7.3 |
|
| Table 5 Length
of stay in hospital by ages |
|
Accidents occurred mainly at home (61%),
affecting women and people at extreme ages. This value is somewhat lower than that
reported by Lyngdorf (Lyngdorf, 1987). Otherwise, adult males were more commonly injured
at work. This distinct distribution is statistically significant at p --0.000001.
Scalding and fires were also in our experience the most frequent cause of burns. These two
account for 70.3% of the whole number. Children were most commonly involved by scalding,
usually due to kettles and pots in the kitchen or to tapwater scalds. Elderly patients
above 70 yrs were in particular burned by flame accidents, typically by domestic fires.
Electrical and chemical burns affected the working population, and the use of fireworks as
a means of entertainment by teenagers and youngsters at local festivities and celebrations
caused many burns. The worst accidents were those occurring at fireworks factories due to
sudden blasts.
We do not know why women were more frequently involved in accidents by gunpowder,
electricity or chemical products. Maybe it is due to the fact that they are more
inexperienced with such materials than their male counterparts.
A special chapter in burns regards road accidents, which may provoke burns when a car
catches fire after a crash. The victims are usually young people about 20 yrs old. Related
to motor traffic, the most frequent burns are those provoked by the exhaust pipes of
motorbikes (hot contact), when the patient puts his/her leg against the pipe. We also had
six patients involved in explosions of butane gas, which is used quite frequently as fuel
by taxi-cabs.
Taking into account the location of the injury, scalding affects the upper limbs and
trunk; flames affected every part of the body because of ignition of clothes; exposed
areas, such as the limbs, hands and face/neck, were frequently involved in electrical and
gunpowder accidents, both in children and in.adults. Electrical flashes affected a typical
pattern of face and dorsum of the hands. Hot contact caused burns in the lower limbs,
mainly due to exhaust pipes and heating devices used by the aged (braziers). Chemical
injuries were in our series more frequent in sites other than the hand (lower limbs, face
and neck), as would be expected.
These conclusions have led us to consider several groups to whom the prevention programme
should be addressed in our area:
- the elderly, with especial regard to the use of safer
heating appliances and to the observance of basic rules to avoid domestic fires;
- parents with small children, to avoid in particular scalds
from baths (by checking the water temperature before bathing) and in the kitchen (by
watching children during food preparation and food consumption);
- teenagers and youngsters in relation to the use of
fireworks as an entertainment, In this regard, our local authorities have recently
introduced laws regulating the size and amount of fireworks commercially available;
- the industrial and working population, especially
electricians and chemists;
- motorists, in order to try to minimize unnecessary
fire-risks like the use of butane as fuel for cars (taxis).
RÉSUMÉ. Les Auteurs
présentent les résultats d'une étude retrospective basée sur 9794 patients brûlés
soignés pendant les quatre ans 1985/1988. L'âge moyen était 24 ans et le sexe masculin
constituait 66% des cas. Les brûlures étaient très fréquentes chez les enfants (
>10 ans), particulièrement à cause de l'ébouillantement. Presque 47% des cas
étaient enfants âgés de moins de 15 ans. Les deux causes principales des brûlures
étaient l'ébouillantement et les flammes. Les autres causes significatives étaient la
poudre et l'électricité. Les brûlures causées par les solides chauds, le feu et les
produits chimiques étaient moins fréquentes. Les brûlures massives ont été causées
par les flammes ou par la poudre, et les lésions plus profondes par l'électricité et
les solides chauds. Pour ce qui concerne le lieu des accidents, les brûlures domestiques
ont été causées par l'ébouillantement et par le feu, et les accidents en plein air par
l'emploi impropre de la poudre et par l'électricité (haute tension). Les accidents du
travail affectent les chimistes et les électriciens. Pour ce qui concerne les accidents
de la route et' du travail, la population masculine est plus nombreuse (p <0.000001).
Le visage et le cou ont été atteints plus fréquemment dans le cas des brûlures
causées par les flammes ou les produits chimiques, le tronc et les membres supérieurs
par l'ébouillantement et les flammes, et les mains et les poignets par les lésions
électriques et la poudre. Les brûlures aux organes génitaux ont été causées par la
poudre et l'ébouillantement.
BIBLIOGRAPHY
- Clark W.R., Fromm B.S.: Burn mortality: Experience
at a Regional Bum Unit and Literature review. Acta Chir. Scand. (Suppl), 537: 1-126, 1987.
- Elberg J.J., Schroder H.A., Glent-Masden L., Hall
K.V.: Bums: epidemiology and the effect of a prevention programme. Bums, 13: 391-394.
1987.
- Lyngdorf P.: Epidemiology of severe burn injuries.
Bums, 12: 491-495, 1986.
- Silverstein P., Lack B.O.: Epidemiology and
prevention. In: Boswick J.A. (Ed.), "The Art and science of burn care", 11-19,
Aspen, 1987.
|