Annals of the MBC - vol. 3 - n' 3 -
September 1990
PHYSIOPATHOLOGY OF
THE BURN SHOCK: RESUSCITATION
Gòmez-Cia T., Roa L., Cantero A.
Grupo di Bioingeneria, ETSII, Universidad de Sevilla,
Espaha
SUMMARY. We
present a comparative analysis of different resuscitation protocols for the burn patient,
realized by digital simulation in a simulator of burn patients previously assessed and
published by our research group.
Introduction
Our simulator of burn patients makes
it possible to analyse the modifications in the distribution of fluids and colloids after
the burn lesion.
According to Davies (1975a, b) the problem of the resuscitation of this kind of patient
revolves around the quantification of the loss of fluids, electrolytes and colloids, as a
function of burn extent and depth and of the time interval since the lesion.
Using conventional physiological techniques based on experiments in animals, various
authors have reached different conclusions. This is reflected in the number of different
resuscitation protocols that are currently followed.
We propose an approximation, from the macroscopic and global point of view, to the
physlopathology of the burn and to the effects of resuscitation, by means of the use of
complex models and digital simulation in the study of these phenomena.
Our objective is to analyse the influence of different resuscitation protocols in the
evolution of the burn.
Materials and methods
Among other published works (Roa,
1979, 1982, 1984, 1986b, 1987a, 1987b; G6mez-Cia, 1986), and in the context of this
Meeting, our research group in 1986 designed calculation algorithms for the analysis of
the extravasation of fluids and colloids in burn patients, starting from clinically
available variables, such as the venous haematocrit and the concentration of plasma
proteins (Roa, 1986a).
Later, in 1988, a simulator of burn patients was published with contested results (Roa,
1988).
The pulmonary capillary dynamic and the effects of the lesion of the alveolocapillary
membrane, following inhalation of toxic substances, were later incorporated in the model
(Roa, 1990 in press).
It is beyond the scope of this paper to give a detailed description of the construction
and testing of the simulator of burn patients, which is presented in the above-listed
publications.
The simulator of burn patients enables us to analyse the response of the organism to any
circumstance, thus helping to confirm or reject hypotheses regarding this complex system,
offering predictions about behaviour in conditions that are difficult to observe or
reproduce, and predicting values of variables that are not available clinically or
experimentally.
Results
Let us imagine an average individual.
Partial -thickness burn lesions are simulated in a burned BSA ranging between 25 and 100%,
without resuscitation treatment.
The hypothesis selected, among all those possible, to simulate the thermal lesion in the
model is that:
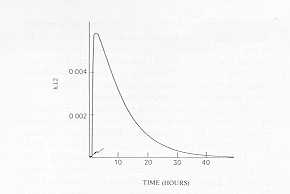
- the burn alters the coefficient of capillary permeability
for the proteins in the burn zone (K12 in' Fig. 1);
- the alteration is greatest between 30 and 90 minutes
post-burn;
- the alteration of K12 diminishes progressively, resuming
initial values approximately 72 h post-burn;
- this alteration is the same for each unit of damaged
capillary surface;
- the gravity of the burn is conditioned by the damaged
capillary surface, which depends on the extent and depth of the burn.
The coefficient of capillary permeability
for the proteins, per unit of lesioned capillary surface, as a function of the time
post-burn, is an original figure.
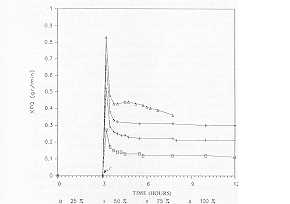
The increase in K12 determines in the organism an increased extravasation of proteins from
the plasma to the interstice in the burn zone (XFQ), related to the lesioned capillary
surface, and therefore to the extent of the burn (25 to 100% in Fig. 2). These results
coincide with those of other authors (Bruhar, 1978; Canaial, 1979, 1980).
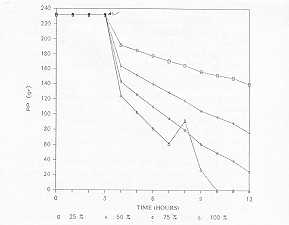
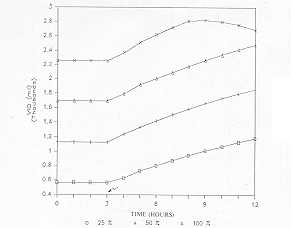
The increased extravasation of plasma proteins leads to their diminution (PP in Fig. 3).
An oscillating behaviour of the PP can be observed in the 100% burned surface area
simulation after 7 h of simulation. It must be remembered that no resuscitation treatment
is administered.
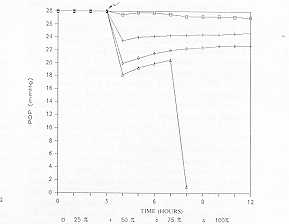
The reduction of PP reduces their concentration in the plasma, and therefore plasma
colloidosmotic pressure (POP in Fig. 4). Here it is worth remembering that, according to
Ley de Starling, POP is the only force that opposes the extIravasation of fluids from the
plasma to the interstice at the capillary level.
At the same time the increased extravasation of proteins to the interstice of the burn
zone increases their concentration, and therefore the interstitial colloidosmotic pressure
in the burn zone (PC1Q in Fig. 5).
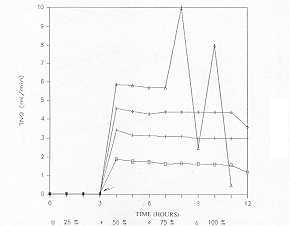
The consequence of a reduction in plasma colloidosmotic pressure post-burn, though
increasing at interstitial level in the burn zone, is an increased extravasation of fluid
from the plasma to the interstice of the lesioned zone (TNQ in Fig. 6). Clinically, oedema
appears at this level. We again observe an oscillating behaviour starting from the 7th h
of simulation in the graph corresponding to 100% burned surface area without resuscitation
treatment.
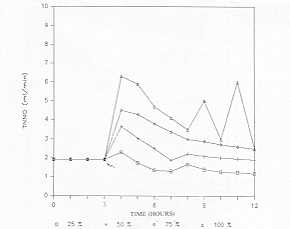
In the healthy area there is also an increased extravasation of fluid (TNNQ in Fig. 7),
initially provoked by the reduction of POP. The oedema at this level would be of
haemodynamic type, with integrity of the capillary membrane.
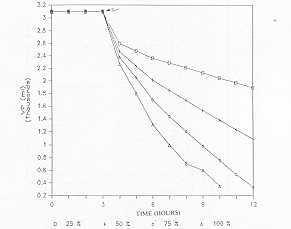
The increased extravasations of plasma to the interstice cause a reduction in plasma
volume (VP in Fig. 8), in relation to the burned surface area. Without resuscitation
treatment, the reduction in VP can be such as to produce hypovOlaemic shock in the burn
patient. The oscillating behaviours mentioned above coincide with a VP lower than 1000
nil.
On the other hand, the extravasation of fluid increases the interstitial volume of the
burn zone (VIQ in Fig. 9). Clinically, oedemas appear which at this level are caused by an
alteration of capillary impermeability (Arturson, 1979).
The organism cannot regulate itself without external intervention, due to the fact that
the interstitial compartment of the burn zone is open exteriorly. This behaviour vividly
underlines the importance of early surgery and of resuscitation treatment that will
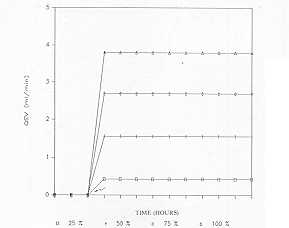
facilitate it. The loss of fluids by evaporation and exudation (QEV in Fig. 10) can reach
dangerous levels (between 4 and 6 1 in 24 h in burns in 75-100% BSA) (Davies, 1974). The
exudate is in addition rich in colloidal substances.
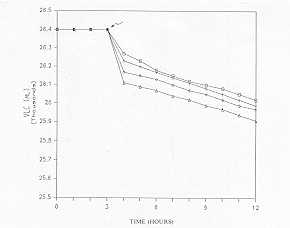
The increase in extracellular osmolarity causes water to pass from the infra- to the
extracellular compartment, reducing the intracellular volume (VLC in Fig. 11). However
this compensatory mechanism is limited and insufficient for the restoration of the losses
caused by the burn. Clinically, there would be intense thirst, and signs and symptoms of
intracellular dehydration with hypovolaernic chock.
We will now analyse the response of the organism to the thermal lesion and to different
resuscitation treatments. The simulation conditions are: average individual, with
intermediate-depth burn in 40% BSA.
The resuscitation protocols analysed are: Parkland (Baxter, 1968), Brooke (Moncrief,
1966), Modified Brooke and Hyperosmolar (Monafo, 1971, 1973, 1976). The Table shows the
infusion rates of fluids and colloids during the first 48 h post-burn in each of the
conditions simulated.
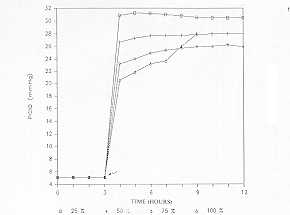
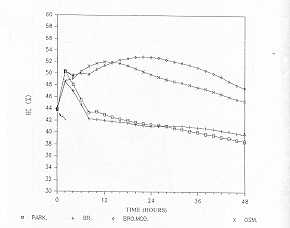
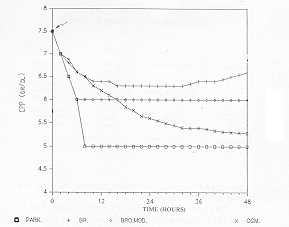
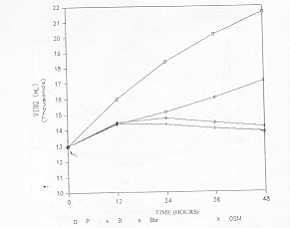
The venous haernatocrit value (HC in Fig. 12), one of the clinically available variables
which provide information about the state of the organism (Roa, 1986), increases in the
post-burn phase, due to the reduction in plasma volume. Starting 3 h post-burn, the
behaviours differ as a function of the amount administered. The Parkland and Brooke
protocols cause a rapid return of HC to its initial values. Both the Modified Brooke and
the Hyperosmolar protocols maintain the same haernatocrits as at the commencement of
infusion, although the return to normality does not occur until the end of the second day,
and slightly elevated values are maintained at termination of the study.
If we analyse the behaviour of the variable constituted by the concentration of plasma
proteins (CPP in Fig. 13), which is also available in routine clinical practice, we find
that after an initial reduction, prior to commencement of resuscitation, the Brooke
protocol prevents a pronounced drop in CPP. Both the Modified Brooke and the Hyperosmolar
protocols are insufficient to maintain CPP. The Parkland protocol even causes a dilution
and reduction of the plasma proteins and of their concentration, thus provoking a drop in
the colloidosmotic pressure of the plasma. We point out the exponential relation existing
between CPP and POP, such that slight variations in the concentration of plasma proteins
cause large alterations in the colloidosmotic pressure of the plasma.
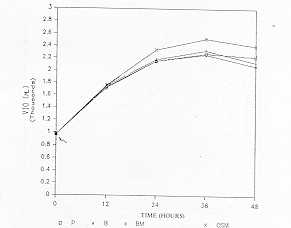
Plasma volume (VP in Fig. 14) is restored in 2 or 3 h after Parkland and Brooke treatment.
Both the Hyperosmolar and the Modified Brooke protocols are insufficient, considering that
although they prevent a greater VP reduction they are unable to restore plasma volume to
approximately normal values.
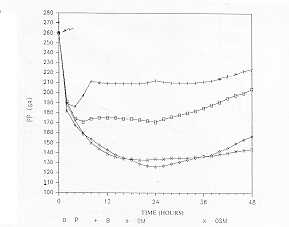
Total plasma proteins (PP in Fig. 15) are restored only with Brooke, in some measure, and
to a lesser extent with Parkland, in the latter case because of a considerable increase in
the lymphatic flow at the level of all the organism.
 |
 |
| Fig. 1 Dynamic
evolution of the variable K12 (coefficient of capillary permeability for proteins in the
burn zone) as a function of A (variable determining the maximum increase of the
coefficient) and B (variable determining the time taken by the coefficient to reach normal
values). In this and all thefiollowing graphs the arrow indicates the occurrence oj'the
burn |
Fig. 2 The
thermal lesion causes at the level of the burn zone an increase in the extravasation of
plasma proteins to the interstice of the burn zone (XFQ) which is in relation to burned
surface area. |
 |
 |
| Fig. 3
The increased extravasation of proteins causes total plasma proteins (PP) to reduce after
the burn lesion. |
Fig. 4 The reduction
in plasma protein concentration post-burn causes a reduction in plasma colloidosmotic
pressure (POP), the only force that tends to reabsorb fluid from the plasmatic to the
interstitial compartment, at capillary level. |
 |
 |
| Fig. 5
The increase in the concentration of interstitial proteins |
Fig. 6 The increase
in interstitial colloidosmotic pressure in the burn zone, together with the reduction in
the plasma colloidosmotic pressure, causes an extravasation of fluid, from the plasma to
the interstice in the burn zone (TNQ), which is considerably increased and proportional to
the damaged capillary surface. |
|
The extravasation of fluid from the plasma
to the interstice in the healthy zone (TNNQ) increases immediately post-burn, being
conditioned by the increase in arterial pressure secondary to the alarm reaction and pain
stimulus caused by the lesion.
 |
 |
| Fig.
7 (CPIQ) causes an increase in the interstitial colloidosmotic pressure in the
burn zone (PC1Q. |
Fig. 8 The
increased extravasation of fluid from the plasma to the interstice is responsible for the
reduction in volume of the plasma (VP). |
 |
 |
| Fig. 9
The interstitial volume of the burn zone (VIQ) increases progressively post-burn.
Clinically, it appears because of the onset of oedema. |
Fig. 10 The
destruction of the cutaneous barrier causes an increase in the fluid lost from the
plasmatic to the interstitial compartment (QEV), in proportion to the burned surface area. |
 |
 |
| Fig. 11
The post-burn behaviour of the interstitial volurne (VLC) is characterized by its
reduction, secondary to the cell destruction caused by the burn. It must be remembered
that the real fluid losses post-burn are isotonic with the plasma; no considerable
alteration of the osmotic balance should therefore occur. |
Fig. 12 Dynamic
behaviour of the venous haematocrit variable (FIC), obtained by simulation, in a patient
of average characteristics with a 40% BSA bum, in whom administration of resuscitation
fluids begins 3 h post-burn (Park. = Parkland, Br. = Brooke, Bro. Mod. = Modified Brooke,
OSM = hypertonic solutions). |
 |
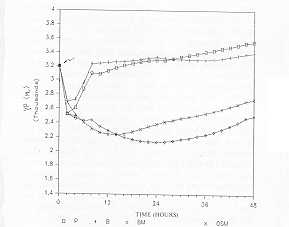 |
| Fig.
13 The Brooke prot. maintains CPP near to normal values. The others are not
effective as regards CPP. |
Fig. 14 After
initiation of resuscitation, both the Parkland and the Brooke protocols boost the
diminished plasma volume (VP), The Modified Brooke and the hypertonic solutions are both
inadequate, although they succeed in maintaining the same VP value as at the beginning of
resuscitation. |
 |
 |
| Fig. 15 Total
plasma proteins (PP) return to almost normal values with the Brooke protocol, remain at
the same level as at commencement of therapy with Parkland, and remain diminished ,
although with a lesser gradient, with Modified Brooke and hypertonic solutions. |
Fig.
16 The burned interstitial volume (V1Q) has a dynamic behaviour, obtained by
simulation, characterized by its being practically independent of the type of resuscitation
utilized. |
 |
 |
| Fig. 17 The
interstitial volume of the healthy zone (VINQ) is related to the quantity and quality of
fluids administered in resuscitation; it increases enormously with Parkland and to a
lesser extent with hypertonic solutions; the behaviours with Brooke and Modified Brooke
are similar, being characterized by a moderate increase. |
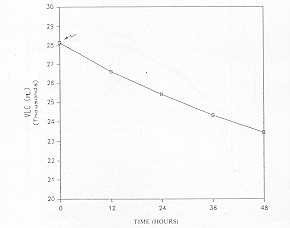
Fig.
18 The dynamic behaviour of the intracellular volume variable (VCL), obtained by
simulation after the administration of hypertonic solutions, is characterized by a
continued reduction. |
|
| |
0-24 h |
24-48 h |
Solution |
| Parkland |
4 ml x kg x %BSA
- |
1/2
50 ml/6 h |
Ringer Lactate
Albumin 20% |
| Brooke |
1.5 mt x kg x %BSA
0.5 ml x kg x %BSA
2000 ml |
1/2
1/2
2000 ml |
Ringer Lactate
Plasma
Glucose 5% |
| M. Brooke |
2 ml x kg x %BSA
2000
- |
1/2
2000 ml
50 ml/6 h |
Ringer Lactate
Glucose 5%
Albumin 20% |
| Hyperosm. |
2 ml x kg x %BSA
- |
2 ml x kg x %BSA
50 ml/6 h |
R.L. (600mOsm/l)
Albumin 20% |
|
Table Simulated
Resuscitation Protocols |
|
The interstitial volume of the burn zone
(VIQ in Fig. 16) is independent of the resuscitation treatment to which the patient is
subjected, and its dynamic behaviour is conditioned almost exclusively by the lesion,
being characterized by a sudden and stable increase.
In contrast, the interstitial volume in the healthy zones (VINQ in Fig. 17) depends to a
large extent on the resuscitation treatment (Hilton, 1981; Roa, 1987a). The Parkland
protocol, which as we saw above maintains in this experiment some circulating plasma
volumes near to normality, determines an enormous increase in VINQ, from 13000 ml to 22000
after 48 h. The cause of this increase is the alteration of the capillary dynamic at a
general level as a result of the reduction in POP. Clinically, this condition occurs
because of the appearance of generalized oedema in patients resuscitated with this
procedure. The oedema wou Id be of haemodynamic type and of iatrogenic origin, expanding
non-selectively throughout the extracellular space. This generalized oedema may be
responsible however for a deficient tissue oxygenation, as also for disturbances such as
metabolic acidosis. Lower increases in VINQ are ,observed with the Hyperosmolar protocol
which, as we saw above, is also insufficient to maintain a plasma volume near to normal
values. The Brooke and Modified Brooke protocols cause less severe oedemas, but only the
former, which contains colloidal substances from the start, is capable of maintaining an
adequate VP. The 50% limit, as the maximum to be used in the calculation of fluids to
infuse according to the Brooke protocol, means that this is insufficient in patients with
burns in more than 60% BSA.
Finally, the use of hypertonic solutions (600 mOsm/I in this experiment) in the
resuscitation of the burn patient causes a reduction in the intracellular volume (VLC in
Fig. 18) in such a continuous manner that it reaches 4.5 L in 48 h of simulation (within
about 15 and 20% of the initial VLC), with the risk of causing latrogenically an
intracellular dehydration.
Conclusion
In our opinion, the techniques of
modelling and simulation, in the context of the classic techniques of burn lesion
investigation (animal experimentation and clinical analysis), are a supplementary working
tool that provide the following information:
- they codify facts and help to confirm or reject hypotheses
regarding complex systems;
- they reveal contradictions between clinical data and
hypotheses;
- they offer predictions of the behaviour of the organism in
conditions that are difficult to observe and reproduce;
- they predict the values of variables that clinically or
experimentally are unobtainable;
- they can suggest the existence of new phenomena.
The results presented regarding the
physiopathology and the effects of resuscitation treatment following the burn lesion may
be summarized as follows:
- resuscitation of the burn patient with colloid-free
solutions reduces the concentration of plasma proteins, and therefore the colloidosmotic
pressure of the plasma, provoking generalized iatrogenic haemodynamic oedema;
- the thermal lesion alters capillary permeability in the
burn zone, and an oedema appears that is not significantly modified by the resuscitation
treatment used;
- the net extravasation of proteins from the plasma to the
interstice of the burn zone is zero starting 12 to 18 h post-burn, since - although
capillary permeability has not been restored - the return of proteins by the lymphatic
system compensates for the losses of these molecules;
- the fluid extravasated to the interstitial compartment of
the burn zone is equivalent to the plasma.
On the basis of our above findings and in agreement with
other authors who have analysed the problem (Davies, 1975a, b; Labondter, 1979, Jelenko,
1978, 1979a, b), we recommend in the resuscitation of the burn patient the use of a lower
infusion volume with a higher content of colloid molecules.
RÉSUMÉ. Les Auteurs présentent une
analyse comparative de différents protocoles de réanimation chez le brûlé, réalisée
avec la simulation digitale dans un simulateur de patients brûlés preécédemment
évalué et publié par leur groupe de recherche.
BIBLIOGRAPHY
- Arturson G., Lousson C.E.: Transcapillary transport
after thermal injury. Scand. J. Plast. Reconstr. Surg., 13: 29, 1979.
- Baxter C., Shires T.: Physiological response to
crystalloid . resuscitation. Ann. N. Y. Acad. Sci., 150: 874, 1968.
- Bruhar B., Carvajal H., Linares H.: Bu rn edema and
protein leakage in the rat: I. Relationship to time of injury. Microvasc. Res. 15: 221,
1978.
- Carvajal, H., Linares H., Bruhard B.: Relationship
of burn size to vascular permeability changes in rats. Surg. Ginecol. Obstet., 149-193,
1979.
- Carvajal H., Linares H.: Effect of burn depth upon
edema formation and albumin extravasation in rats. Burns, 7: 79, 1980.
- Davies J., Larnke L., Li1jedhal S.: A guide to the
rate of non-renal water loss from patients with burns. Br. J. Plast. Surg., 27:235,1974.
- Davies J.: The fluid therapy given to 1027 patients
during the first 24 hours after burning. 1: Total fluid and colloid input, Burns, 1/4:
319, 1975a.
- Davies J.: The fluid therapy given to 1027 patients
during the first 24 hours after burning. 11: The inputs of sodium and water and the
tonicity of the therapy burns. Burns, 1/4: 331, 1975b.G6mez-Cia T., Rea L., Lazo M.:
Dynamic analysis of the influence of reanimation treatment in burned patients. The 1986
International Conference of the Systems Dynamics Society, p.,293 Proc., Seville, Spain,
1986.
- Hilton J.: Effects of fluid resuscitation on total
fluid loss following thermal injury. Surg. Gynecol & Obst., 152/4: 441, 1981.
- Jelenko C., Wheeler M., Callaway B.: Studies in
shock and resuscitation. 11: Volume repletion with minimal edema using the
"HALED" method. Jacep 7: 326, 1978.
- Jelenko C., Williams J., Weeler M.: Studies in shock
resuscitation. 1: Use of a hypertonic albumin -containing fluid demand regimen (HALED) in
resuscitation. 1. Crit Care Med., 7:57, 1979a.
- Jelenko C., Solemberger R., Weeler M.: Studies in
shock and resuscitation. III: Accurate refractometric COP determinations in hypovolemia
treated with HALED. Jacep 8: 253, 1979b.
- Labondter H., Wax S., Webb W.: Hypertonie
albuminated (Hal) solution burn resuscitation study. American Burn Association Meeting,
March, 1979.
- Moncrief J.: Effect of various fluid regimens and
pharmacological agents on the circulating haemodynamics of the immediate postburn period.
Ann. Surg., 164: 723, 1966.
- Monafo W.: "The treatment of burns: principles
and practice", W.H. Green Co., St. Louis, 1971.
- Monafo W., Chumtrasakul C., Ayzaviarn V.: Hypertonic
sodium solutions in the treatment of burn shock. Amer. J. Surg., 126: 778, 1973.
- Monafio W., Ayzaviarn V., Logel R., Deitz F., Eve
M.: Renal function after thermal trauma: the effects of treatment on renal blood flow and
sodium and water excretion. Surgery, 79/3: 342, 1976.
- Roa L., Gonzalez F.: Aproximaci6n analitica de
funciones no lineales que apparecen en la modelizaci6n de sistemas fisio16gicos. XI
Reunion de Estadistica Inves. Operat. E InformAtica, p. 8 Proc., Seville, Spain, 1979.
- Roa L.: A model of the transport and distribution of
the bodily fluids using the system dynamic approach. IEEE Computer Soc., International
Conf on Medical Computer Science/Computational Medicine, p. 393 Proc., Philadelphia, USA,
1982.
- Rea L., Trulillo F., Rodriguez M., Gonzalez-Baron
S.: Nonlinear analysis of arterial pressure. Rev. Esp. Fisiol., 40: 325-332, 1984.
- Roa L., G6mez-Cia T.: Analysis of the extracellular
protein and fluid shifts in burned patients. Burns, 12: 337, 1986a.
- Roa L., G6mez-Cia T., Gonzalez-13aron S.: Computer
model of dynamic capillary control system. IV Mediterrancam Conference on Medical and
Biological Engineering, Mecombe 86, p. 130 Proc., S.eville, Spain, 1986b.
- Roa L., Cantero A., Lazo M.: Algorithme d'analyse de
la formation de l'oedème chez les grands brûlés. ITBM, 8: 134, 1987a.
- Roa L., G6mez-Cia T., Cantero A.: Mathematical model
for digital simulation of a burn injury. Genova International Congress on Burn Injuries,
p. 3 B06 Proc., Geneva, Switzerland, 1987b.
- Rea L., G6mez-Cia T., Cantero A.: Analysis of burn
injury by digital simulation. Burns, 14: 201, 1988.
- Webb W. R., Brunswick R. A.: Microcirculation i n
Shock -Clinical Review, in "Path op hysiology of Shock, Anoxia, and Ischernia",
Cowley R.A., Trump B.F. (Eds.), Williams & Wilkins Co., Baltimore, USA 1982.
|