Annals of the MBC - vol. 3 - n' 3 -
September 1990
SURGICAL TREATMENT
OF POST-BURN LEUK0DERIVIA
El-Otiefy M.A., EI-Sonbaty M.A.
Plastic Surgery Unit, Department of Surgery Faculty of
Medicine, Assiut University, Egypt
SUMMARY. Post-burn leukoderma is
one of the common complications of bums which usually lead to social and psychological
disturbances. Its treatment can be difficult. 30 patients with post-burn leukoderma have
been studied and surgically treated with excision and skin grafting for the last 3 years
in our Plastic Surgery Unit. Modifications of the technique were developed during their
treatment. The results were encouraging as regards cosmetic appearance.
Introduction
Pigmentation is not only a protective
function of the melanocyte but also plays an important role in cutaneous aesthetics
(Fitzpatrick, 1971).
Leuko~erma is the outcome of specific disorders or conditions and ill-defined factors
affecting the pigmentary system through either local destruction or absence of
melanocytes, and sometimes through inhibition of their function. Although leukoderma is a
clinically benign disorder, psychological and social consequences are common (Porter et
al., 1979).
Replacement of the affected epidermis with a graft bearing functional melanocytes will
improve the cosmetic problems. Such a technique, known as epidermal grafting, was first
described by Falabella in 1971.
The aim of this work is to extend experience of repigmentation of post-bum leukoderma by
autologous split-thickness skin grafts and to describe a few improvements in the
techniques.
Materials and methods
This study included 30 patients with
post-burn leukoderma who presented to our Plastic Surgery Unit during the last 3 years. 9
were males and 21 were females. Their ages ranged from 7 to 55 years. Most of their
leukodermic areas were in the upper and lower limbs and the front of the chest (Table).
Two-thirds of these patients had post-burn contractures in addition to their leukoderma.
For these patients correction of their contractures took the first priority, followed by
treatment of the leukoderma.
The other one-third of the patients had post-burn leukoderma only, and they presented in
order to have their unsightly white areas treated.
Scalped excision of the leukodermic areas was practised in 12 cases (Fig. 1). Tangential
skin excision of the leulcodermic areas using a skin graft knife was performed in 13 cases
(Fig. 2). Combination of the two methods of skin excision was eftected in 5 cases.
The split-thickness skin grafts used to cover the resultant raw surfaces were taken from
normal skin donor sites in 17 cases and from healthy uncomplicated previous donor sites in
13 cases.
The last modification in our work was use of the previously treated leukodermic areas as
donor sites of skin graft to show whether it retains or loses its pigmentation (Fig. 3).
Discussion
Unsightly leukoderma mainly on exposed
skin surfaces is a common complication of burns. Patients with burns usually accept
hyperpigmentation more than leukoderma.
There are several reports (Falabella, 1978; Kono et al., 1963) that vitiligo vulgaris can
be repigmented successfully with multiple minigrafts. Harashina (1985) reported the
treatment of leukoderma after bums by a combination of dermabrasion and chip skin grafts.
In the present work, we used the previously reported use of skin graft in the treatment of
post-burn leukoderma, but during the period of work there were modifications in this
conventional method.
Scalpel excision of the leukodermic areas was usually time-consuming, associated with much
bleeding, and resulted in widening of the defects. The skin grafted areas were subject to
contractures unless sufficiently splinted. Epidermal excision of the leukodermic areas
therefore replaced scalpel excision and it was observed that epidermal excision was a
rapid procedure, associated with less bleeding. No widening of the treated areas occurred
and after its covering by skin grafts, there was no hazard of contractures, since the
dermis remained unharmed.
 |
 |
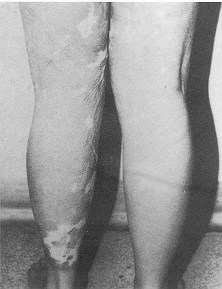
| Fig. 1 Female
patient aged 20 years with post-burn leukoderma in front of the knee and leg. a)
pre-operative, b) post-operative after scalpel excision and S.S.T.G. |
 |
 |
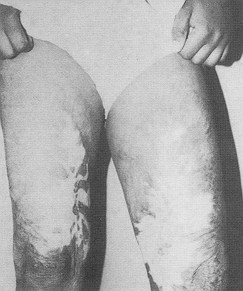
| Fig. 2 Female
patient aged 14 years with post-bum leukoderma of inner side of both thighs. a)
pre-operative b) immediate post-operative after tangential skin excision and S.S.T.G. |
|
 |
 |
 |
 |
| Fig. 3 Female
patient aged 16 years with post-bum leulcoderma a) pre-operative b) post-operative; the
treated leukoderma was used again as a donor site in the left thigh c) pre-operative d)
post-operative, using the skin taken from the treated leukoderma. |
|
Hyperpigmentation used to be one of the
problems afTecting skin grafts (Miry Mir, 196 1), until a method of skin grafting
utilizing previous donor areas was reported by Lopez, in 1972. This method seems to
produce less pigmentation of the grafts. Using previously healed uncomplicated donor sites
as a source of skin graft, the results were cosmetically encouraging as regards the colour
of the grafts.
For patients with extensive post-burn leukoderma and limited donor sites, we can harvest
the same donor sites more than once. Also the grafted leukodermic areas can be used as an
additional donor site with accepted cosmetic appearance.
RÉSUMÉ. La
leucodermie est une complication commune des brûlures qui crée très fréquemment des
problèmes sociaux et psychologiques. Le traitement peut être difficile. Pendant une
période de 3 ans les Auteurs ont étudié chez leur Unité de Chirurgie Plastique 30
patients qui présentaient la leucodermie post-brûlure, soumis à l'excision chirurgicale
et à la greffe cutanée. Au cours du traitement certaines modifications de la technique
ont été développées. Les résultats ont été encourageants pour ce qui concerne
l'aspect cosmétique.
BIBLIOGRAPHY
- Falabella R.: Epidermal grafting: An original
technique and its application in a chronic and granulating areas. Arch. Dermatol., 104:
592-600, 1971.
- Falabella R.: Repigmentation of leukoderma by
minigrafts of normally pigmented autologous skin. J. Dermatol. Surg. Oncol., 4: 916-919,
1978.
- Fitzpatrick T.: Melanocyte system. In: Fitzpatrick
T.B. et al. (Eds.), "Dermatology in General Medicine", 117-146, McGraw-Hill, New
York, 1971.
- Flarashina T. Ryosyke I.: The treatment of
leukoderma after burns by a combination of dermabrasion and chip skin grafting, Br. J.
Plast. Surg., 38: 301-305, 1985.
- Kono K., Nozaki T., Sawada H., Ohashi M.: The
spotted skin grafting method on vitiligo vulgaris. Journal of the Japanese Dermatological
Association, 73: 67, 1963.
- Lopez-Mas J., Ortiz-Monasterio F., Vialede Gonzales
M., 01mcdo A.: Skin graft pigmentation, a new approach to prevention. Plast. Reconstr.
Surg., 49: 18-21, 1972.
- Miry Mir L.: The problem of pigmentation in the
cutaneous graft. Br. J. Plast Surg., 14: 303-307, 1961.
- Porter J., Beuf A. J., Nordlund J.J.: Psychological
reaction to chronic skin disorders. A study of patients with vitiligo. Gen. Hosp.
Psychiatry, 1: 73-77, 1979.
|