Annals of the MBC - vol. 3 - n' 4 -
December 1990
THE
TREATMENT OF BURN SCARS: OUR EXPERIENCE
loannovich J., Panayotou R., Mantas N., Alexakis
D.
Center of Plastic Surgery and Microsurgery,
General State Hospital of Athens, Greece
SUMMARY. Scar evolution leads to
three possible abnormalities: scar contractures, hypertrophic scars and keloids. As the
quality of a scar is however unpredictable, preventive measures, including the use of
fatty ointments and continuous pressure, should always be taken. Splints are also useful.
The treatment of the three main abnormalities is described. No method is perfect and the
aim in the treatment of burn scars must therefore be the prevention of abnormalities by
early excision of the primary bum wound.
The scar is the end result of wound
healing in the deep partial thickness and full thickness burns. According to its
pathology, scar evolution leads to the formation of three different types of abnormality:
- scar contractures
- hypertrophic scars
- keloids.
The evolution of the scar depends on
various factors, of which some can be altered by therapeutic measures. Others can
influence the quality of the scar in a negative way, such as the site of the scar, its
healing process, the age, sex and race of the patient, etc. (Peacock and Winkle 1976).
Nevertheless, the quality of a scar is unpredictable, especially for the first 10-15 days
after its appearance. For this reason preventive measures should be undertaken in time to
avoid the manifestation of an abnormal scar (Tab. 1).
The experimental trials of Ohura (1989) have recently demonstrated that fatty ointments
penetrate easily into the scars and the surrounding normal skin. It seems that the
maintenance of a fatty milieu around the scar diminishes the period of aseptic
inflammation and excludes irritation by the exfoliation of the new scar.
Many observations reveal that from the preventive point of view the combination of this
treatment with continuous pressure has encouraging results, especially in extended burn
scars.
Pressure does not allow the formation of interstitial oedema and restricts the development
of new capillaries, when applied in a range of 15-40 min Hg (Harries and Pegg 1989).
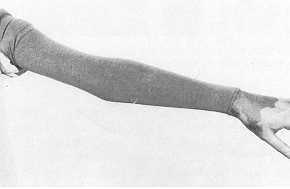
For this purpose the well-known garments have been invented (Figs. 1, 2). They should be
applied two weeks after grafting or when spontaneous healing has occurred. They should be
worn for 9-12 months, all day long, until the scars become soft, flat and pale in colour.
Although compression was first described by
A. IMMEDIATE POSTOP.
MANAGEMENT OF A SCAR
(PREVENTIVE MEASURMENTS)
- Application of fatty and/or cortisone containing ointment
and creams
- Reduction of skin tension
- Application of continuous compression
- Splinting
|
Dupuytren in 1832 there is still some
controversy regarding its mode of action and even of its necessity. In our department we
routinely use the combination of ointment and pressure garment treatment for at least 9-12
months for scars in all parts of the body, except the face, where the application of
garments is not easily tolerated by our patients.
|
Fig.1
Pressure garment for the upper extremity. |
|
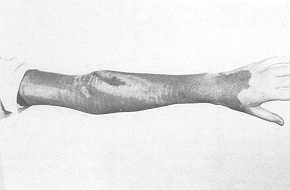
Fig.2
Flattened bum scar obtained after application of the pressure garment for a two-month
period. |

|
Fig.3
Special splint for prevention of scar contracture in neck region after skin grafting. |
|
Preventive measures for scar formation,
especially after skin grafting, include the use of splints, particularly in the neck, the
upper extremities and hands. They lead, through immobilization, to a softening of the
scar. Immobilization in an extreme extension position, as in burns of the neck, leads to
diminished contracture (Fig. 3).
Scar contractures
In burns, contracture usually appears
when the scar line is vertical to the skin tension lines, as in scars over a joint. It
should be emphasized that the primary treatment of the burn wound should actually aim to
diminish scar contracture by grafting the patients as soon as possible. In some cases
pediele flaps or even free flaps can be used primarily to cover the defect and prevent
contracture.
The treatment of choice for scar contracture is scar revision, combined with another
surgical procedure, according to the localization, extent and shape of the scar. For
example, Z-plasty can redirect the scar and reduce skin tension (Fig. 4 a, b). If on the
other hand the scar contracture leads to a restriction of the full range of motion, skin
grafting or the use of a flap is indicated to cover the tissue defect.
Tissue expanders can be used today in different shapes and volumes as a secondary
procedure to reconstruct defects (Fig. 5 a, b). We do not use tissue expansion for a
primary closure of an open wound: In severe contractions skin grafts still give as good
results as the myocutancous or fasciocutaneous axial flaps. It is up to the surgeon to
decide which method to use.
Hypertrophic scars
Hypertrophic scars are more commonly
seen in burn wounds. It is clinically very difficult to differentiate them from keloids
arising from bum wounds, although they are different pathological entities.
Hypertrophic scars always develop when the primary excision is delayed more than 10 days
post-bum. Due to aseptic inflammation, it is not advisable to operate before the first 8
months, unless the scar causes functional disorders. Meanwhile, in our department, we
apply various conservative measures, depending on the scar extent.
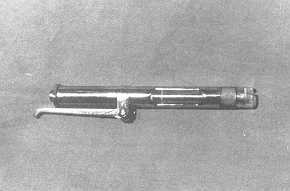
Localized scars of small extent are treated with steroid injections. We have found that
the use of an air-jet apparatus ("dermo-iet") is more efficient than the
injection with an ordinary needle (Fig. 6). With such a needle it is more or less
impossible to inject the medicament intralesionally, because of the fibres' density. The
jet-apparatus has the property of having the appropriate pressure, and the moment of
"firing", to insert the medicament intralesionally. It seems that the main
advantage of the dermo-jet lies in the pressure, which causes a destruction of the
irregularly woven fibres. It seems that steroids are also necessary, although it causes a
destruction of the fibres. According to our policy we estimate the response to the
treatment after the second session, when the hyperti-lophic scar becomes softer and
itching disappears. The treatment continues in sessions till the scar becomes thinner and
softer. The colour change is the last of the symptoms to be restored and is observed some
months after the treatment is finished.
|
 |
Fig.
4 Narrow axillary contracture (a), corrected by the use of multiple Z-plasty (b).
|
|

|
 |
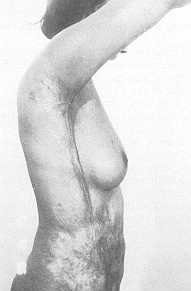
Fig.
5 Hypertrophic bum scar on the elbow area (a), and (b) the position of a
rectangular tissue expander under the adjacent healthy skin for a latter reconstruction of
the scar. (The tissue expander is partially inflated.) |
|
|
Fig. 6 The
air-jet apparatus. (Dermo-jet, Model G-Robbins Intruments Inc., Chatham, N. Jersey) |
|
The surgical treatment varies depending on
the extent and the site of the hypertrophic scar. Small scars can be revised and removed,
the defect being covered by local or distant flaps. In extensive scars tension should be
released primarily, because the scar will not soften and more importantly constant
irritation may lead to the formation of precancerous lesions. The defects resulting from
the relief of tension are covered by split thickness skin grafts, which in some cases are
meshed.
Small and multiple hypertrophic scars should be treated by dermabrasion (Schreuss 1949,
1965). We avoid applying this method during the late spring and summer time, since sun
irradiation in our country can result in deeper coloured areas of the skin. In our
experience the results are not very satisfactory when dermabrasion is applied to patients
of darker skin, since it results in a whitish skin area.
Keloids
Our experience in the treatment of keloids is limited,
since in our population their incidence is very low. Irradiation (Chaoul's intensive
irradiation) should not be considered the therapy of choice 'in benign lesions and in
particular in keloids, because of its serious side effects. The combination of excision
and post-operative irradiation seems to have good aesthetic results without being of any
harm to the patient (Schumacher 1972).
The. application of continuous compression as well as of steroids is unfortunatelly not
efficient for the treatment of keloids.
The use of the C02-laser to excise the keloid combined with local compression has been
recently applied but the results are not encouraging (Apfelberg 1987).
The removal of the keloid and coverage of the defect with skin grafts or flaps, combined
with continuous compression, seem to be the method which brings the most satisfactory
results, and the fewest recurrences.
In conclusion, the treatment of scars cannot be generalized and should always be
individualized for each patient. It should be stressed that our efforts to treat bums must
always include the consideration of facing a future disfiguring or disabling scar.
It is evident that none of the above methods gives perfect results. For this reason the
main aim in the treatment of burn scars is to limit their development by performing an
early excision of the primary bum wound.
RÉSUMÉ. L'évolution des cicatrices porte
à trois abnormalités possibles: les contractures cicatricielles, les cicatrices
hypertrophiques, et les chéloïdes. Puisque la qualité de la cicatrice est toujours
imprévisible, il faut en tout cas adopter des mesures de prévention, comme par exemple
l'emploi d'onguents grais et la pression continuelle. Les échelles sont aussi utiles. Les
auteurs décrivent le traitement des trois types principaux d'abnormalité. Il n'existe
pas de méthode parfaite et le but du traitement des brûlures doit être pourtant la
prévention des abnormalités à travers l'excision précoce de la zone primaire brûlée,
BIBLIOGRAPHY
- Apfelberg D.B.: "Evaluation and installation of
surgical laser systems". Springer Verlag, Berlin, 1987.
- Harries C.A., Pegg S.P.: Measuring pressure under
bums pressure garments using the Oxford pressure monitor. Bums, 15: 187, 1989.
- Ohura T.: The kinetics and the effect of
antibacterial agents administered systematically or topically to the bum wound. III
Congresso Argentino de Quemaduras, Buenos Aires, 1989.
- Peacock E.E., V. Winkle W.: "Wound
healing". Saunders, London,1976.
- Schreuss H.T.: Hochtouriges Schleifen der Haut.
Zschft. Hautkrkhtn. 8: 151, 1950.
- Schreuss H.T.: Fraesen und Schleifen. In: Gohrbandt
et al.: "Handbuch der Plastischen Chirurgie". De Gruyter Verlag, Berlin, 1965.
- Schumacher W.: Die Strahlenbehandlung im Rahmen der
Narbenbehandlung. In: Gohrbandt et al.: "Handbuch der Plastischen Chirurgie". De
Gruyter Verlag, Berlin, 1972.
|