Annals of the MBC - vol. 3 - n' 4 -
December 1990
A
RETROSPECTIVE STUDY OF 5505 BURNED PATIENTS ADMITTED TO ALEXANDRIA BURNS UNIT
Mostafa M.F., Borhan A., Abdallah A.F., Beheri
A.S., Abul-Hassan H.S.
Department of Plastic and Reconstructive Surgery
and Burns, Alexandria Faculty of Medicine, University of Alexandria, Egypt
SUMMARY.
5505 burned patients were retrospectively studied from 1969 to 1981. Most patients were
young (10-30); 40.05% of the cases had less than 10% surface area burn. Scalds represented
the most common cause of burns, followed by flames. The bums were mostly domestic in
origin with an overall mortality rate of 21.1%, with causes such as acute renal failure,
pneumonia, septic shock, acute gastric ulcerations and bleeding. The average hospital stay
was 33.2 days.
Introduction
Since the dawn of history bum wounds
have been recognized as one of the most serious injuries a living body can sustain. They
have received attention and the most thoughtful thinking throughout history: a thinking
which has varied from a real factual approach to the extreme of witchcraft. The need for
specialized care and lines of management has encouraged many institutions to culminate
these efforts in well-organized and equipped Burns Centre. The Alexandria Burns Centre,
started in 1969, was recognized as the first highly specialized Burns Centre in the Middle
East. In spite of the fact that expansion in this Centre is very expensive and tedious,
our Unit, which started with 15 beds, had grown into a 28-bed unit by the end of 1976.
Recently, at the end of 1988, another unit with a total capacity of 30 beds was opened in
the same hospital.
This retrospective study will cover the activity in bums care during the period 1969-1981,
with an overall number of 5505 patients admitted to the Burns Unit.
Review of data
5505 patients who sustained different
types of burns Were admitted to the Unit from 1969 to 1981. The mean admission was 544
patients per year, 45.3 patients per month and 1.3 patients per day (Fig. 1). Scalds
constituted 51.6% of the total causes of burns, and flames 46.9%. Electrical burns were
0.98% and chemical burns 0.45% (Tables 1 and 2). The age group 10-19 years was the largest
age group and that of 60 years and over was the smallest.
The surface area burned varied according to the cause. It was limited in scalds and
extensive in flame burns. Patients, with surface area burned (SAB) from 0-9% represented
40.25%, whereas those with 10-19% constituted 26.17% of the whole number of admissions.
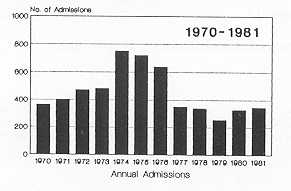 |
Fig. 1 - Annual admission to the
Alexandris Burns Unit from 1970 to 1981 |
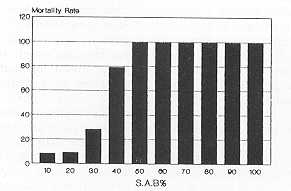 |
Fig. 2 - Mortality rate according
to S.A.B. % |
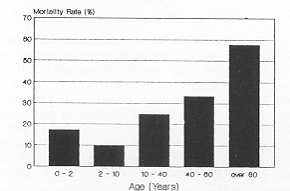 |
Fig. 3 - Mortality rate according
to age |
|
During the period included in the study,
1182 patients died, with an overall mortality of 21.1% (Table 4). This overall mortality
was found to increase with the extent of SAB. In the group of patients suffering from a
30-39% SAB, the mortality rate was 20.5%, and in those with 40-49% it was 40.4%. The death
rate was almost 99% in patients with more than 60% SAB. In the recent data, this figure
will be expected to improve with the advent of early tangential excision and skin grafting
as a routine technique in our Unit (Fig. 2).
Mortality rate in relation to age is demonstrated in Table 4, with the highest rate in
patients above 60 years (57.5%) compared to children less than 2 years (17.1%) (Table 4
and Fig. 3). The mean stay in hospital, after exclusion of deceased patients and of those
with bums in less than 10% SAB, was 33.2 days; if the group of < 10% SAB is included,
the mean stay in hospital drops to 15.5 days per patient.
Septicaemia was the commonest cause of death in deep and extensive bums in this study.
Acute renal failure was the caus e of death in patients dying in the very early days after
injury.
Discussion
The annual total admission to the
Alexandria Burns Unit is on the increase, as demonstrated by the expansion in the total
number of available beds for bum patients from 1969 to 1988 (11, 12). This is in spite of
the fact that other hospitals in Alexandria started to receive these critical patients in
their units. The average admission rate per year was 544 and if an average of 25% of cases
was admitted to other hospitals, the average admission rate in Alexandria was about 681
patients, which means almost 340/million (12).
The review of causes, age, and sex distribution reveals valuable data, as we found that
scalds affected 51.6% of our patients. 91.6% of these cases were children below two years
of age with equal sex bums, females were almost double the number of males. This can be
explained by the high number of suicide attempts due to psychological and social troubles.
Accidental flame bums are due to the misuse of kerosene or butane stoves and to the
carelessness of people wearing synthetic clothes near these stoves. Epileptics and feeble
elderly patients represented the remainder of this group of flame burns, with the addition
of a few cases of homicidal flame bums (compared to 25% of such cases reported before) (4,
5).Flame burns affected 46.9% of the series, 67.9% of this figure being adults. In this
group of flame
Year |
Number of
Patients |
1969 |
78 |
1970 |
361 |
1971 |
399 |
1972 |
470 |
1973 |
480 |
1974 |
751 |
1975 |
718 |
1976 |
639 |
1977 |
348 |
1978 |
338 |
1979 |
253 |
1980 |
326 |
1981 |
344 |
Total |
5505 |
|
Table 1 - Yearly
admission rate to the Alexandria Burns Unit |
|
Cause of
Burn |
Number of
Patients |
Percentage |
Scalds |
2842 |
51.62 |
Flame |
2585 |
46.95 |
Electrical |
54 |
0.98 |
Chemical |
24 |
0.45 |
Total |
5505 |
100.00% |
|
Table 2 - Causes
of burn in 5505 patients |
|
| SAB |
Scalds |
Flame |
Elect. |
Chern. |
No. |
% |
| 0 - 9 |
1682 |
477 |
31 |
15 |
2205 |
40.05 |
| 10 - 19 |
847 |
579 |
10 |
5 |
1441 |
26.17 |
| 20 - 29 |
205 |
390 |
6 |
1 |
602 |
11.04 |
| 30 - 39 |
72 |
271 |
3 |
2 |
348 |
6.32 |
| 40 - 49 |
17 |
166 |
1 |
1 |
185 |
3.36 |
| 50 - 59 |
5 |
154 |
- |
- |
159 |
2.88 |
| 60 - 79 |
3 |
134 |
1 |
138 |
2.50 |
- |
| 70 - 79 |
8 |
137 |
1 |
146 |
2.65 |
- |
| 80 - 89 |
- |
109 |
1 |
110 |
1.99 |
- |
| 90 - 100 |
3 |
168 |
- |
- |
171 |
3.04 |
|
Table 3
in the four types of burn |
|
| Age per Year |
No. of Cases |
No. of
Deaths |
Mortality
Rate (%) |
| 0 - 2 |
731 |
139 |
17.1 |
| 2 - 10 |
2035 |
197 |
9.7 |
| 10 - 40 |
2817 |
703 |
24.6 |
| 40 - 60 |
291 |
97 |
33.3 |
| over 60 |
80 |
46 |
57.5 |
| Total |
5505 |
1182 |
21.1 |
|
Table 4
Relation between mortality and age |
|
In England and Wales, when the causes of
bums have been analysed, it has been concluded that most accidents are of the domestic
type with more flame bums than scalds (10, 14). While children are the victims in most
scald bums, females are affected in direct and indirect flame burns. These data are
different from our review in many aspects (2, 10-12). Electrical (19 and chemical (4~ bums
constituted a minority of our admissions, only 0.9%. This can be explained by the fact
that most of the victims of these cases were workers in factories who were usually
transferred to Health Insurance Hospitals.
Several recent reviews on bum mortality from regional centres have shown an encouraging
increase in survival rates and a significant decrease in hospitalization time (6, 7). For
instance, Curreri reviewed his past 16 years of experience and reported a survival rate of
63% for patients aged 15-44 years (5). This improvement may be attributed to increased
clinical and laboratory research on the diagnosis and treatment of bum shock, inhalation
injury, infection, nutrition and wound coverage (7, 8, 19, 20). Marshal and Dimick (9), in
reviewing their large series, note correctly that mortality is not only related to the
size and depth of bum, but markedly increases with subsystem failure, such as cardiac,
pulmonary, or renal. Mortality rates were demonstrated in different studies by Tumbsch
(20.5%) (22), Pruitt (16.9%) (16), and Rittenburry (24.9%) (17). These studies are
comparable to our data of a 21.1% overall mortality rate (12).
Burned children carry a higher risk, because they are fragile and have low resistance to
injury and usually die from dehydration, bronchopneumonia or septicaemia. Our series shows
a mortality of 8.2% in children under 10 years. This is comparable to Ryan's study, with
10.9% for children below 3 years, and less than 10% SAB (18), while Mc Dowall calculated
an incidence of 3.7% mortality rate in children in his series (10).
Older age groups had higher rates of death, as shown in other studies that showed a 57%
death rate, compared to 56.5% in our study (6).
The commonest causes of death in our series were acute renal failure during the early days
of treatment, pneumonia and bronchopneumonia, especially in infants and children, and
septic shock, particularly in deep extensive burns. Pulmonary burns, bums of the
respiratory passages, pulmonary embolism, and severe haematemesis due to gastrointestinal
ulcerations were other causes of less importance.
Phillips and Cope (15) studied the causes of death in Massachusetts General Hospital and
found that shock caused 20% of deaths. Respiratory tract damage with or without
respiratory tract infection caused 50% of deaths. Wound sepsis did not appear to represent
a major cause of death, in contrast to our study. Other studies have demonstrated the
effect of bronchopneumonia and septicaernia as the main causes of death (16).
In our series, the mean stay in hospital was 15.5 days if all patients admitted were
considered and fatalities excluded. However, this figures rises to 33.2 days if deaths and
cases with less than 10% SAB are excluded. This is to be compared to studies by Colebrook,
with an average of 50 days' stay in hospital (3). Muir and Barclay reported a period of 6
weeks as the mean stay in hospital (14), while in Denmark (2 1) and Chile (20) the mean
stay in hospital was 20 and 26.8 days respectively.
With the advent of tangential excision in extensive cases of deep-thickness bums (8), the
mean stay in hospitals is expected to reach the figures reported by Curreri (5).
RÉSUMÉ. Les
Auteurs présentent une analyse rétrospective de 5505 patients brûlés hospitalisés
pendant la période 1969-1981. La plupart des patients étaientjeunes (10-30 ans); dans
40.05% de cas les brûlures couvraient moins de 10% de la surface corporelle. Les
ébouillantements représentaient la cause plus commune des brûlures, suivie par les
flammes. Le plus souvent les brûlures avaient une origine domestique. Le taux complessif
de mortalité était 21,1%; les causes du décès les plus fréquentes étaient
l'insuffisance rénale aiguë, la pneumonie, le choc septique, les ulcérations gastriques
aiguës et l'hémorragie. La période moyenne d'hospitalisation était 33,2 jours.
BIBLIOGRAPHY
- Artz C.: Changing aspects of electrical injury. Am.
J. Surg., 128: 600, 1974.
- Cogswell I., Chu A.C.: Severe bums in children
1964-1975. Arch. Dis. in Childhood, 51: 67, 1976.
- Colebrook L. Colebrook V.: A suggested national plan
for reducing bums. Lancet, 2: 579, 1951.
- Crikelair G., Symonds F., Ollestein R.: Bum
causations, its many sides. J. Trauma 8: 572, 1968.
- Curreri P.W., Luterman A., Braun D.W., et al.: Bum
injury.Ann. Surg. 192: 472, 1980.
- De Meestre T., Feller I.: Mortality in burned
patients 61 years of age and older. Surg. Gynec. Obstet.; 126: 1041, 1968.
- Demling R.H.: Improved survival after massive bums.
J.Trauma, 23: 179, 1983.
- Janzekovic J.: A new concept in the early excision
and immediate grafting of burn. J. Trauma, 10: 1103, 1970.
- Marshall W.G., Dimick A.R.: Natural history of major
bums with multiple subsystem failure. J. Trauma, 23: 102, 1983.
- Me Dowall A.: A seven-year survey of a bums unit for
children 1954-1960. Br. J. Plast. Surg. 18: 1535, 1965.
- Mostafia M., Borhan A., El-Tahan A., Abdel-Fatah A.:
A retrospective study of 850 burned patients admitted to the Burns Unit of Alexandria
Medical School. Bull. Alex. Fac. Med., 8: 2, 1972.
- Mostafa M., Abdel-Fatah A.: A retrospective study of
3896 burned patients. Transactions of the 7th International Congress of Plastic and
Reconstructive Surgery, Rio De Janeiro, 1970.
- Moyer C.A.: An assessment of the therapy of bums.
Ann. Surg.,137: 628, 1953.
- Muir, Barclay T.: "Bums and Their
Treatment", 2nd ed., 1- 14, Lloyd-Luke Ltd., London, 1974.
- Phillips AW., Cope 0.: Burn therapy. Ann. Surg.,
155: 1, 1962.
- Pruitt B., Tumbusch W.: Mortality in I 100
consecutive bums treated at a burn unit. Ann. surg., 159: 396, 1964.
- Rittenburry M., Maddox R., Schmidt F.: Probit
analysis of bum mortality in 1831 patients; comparison with other large series. Ann.
Surg., 164: 123, 1966.
- Ryan R., Rasmussen J.: Bums in children. Plast. and
Reconstr.Surg., 42: 334, 1968.
- Salisbury R., Holder D.: Burns: Current concepts and
controversies. In: Georgiade and Georgiade, "Essentials of Plastic, Maxillofacial and
Reconstructive Surgery", 195, Williams and Wilkins, 1987.
- Schapiro J.A.: Bums in Chile. In: Research in Bums,
Am. Inst.Biol. Sciences, 9, 37, Blackwell Publications, Oxford, 1962.
- Sorensen B., Thomson M.: The bums unit in
Copenhagen.Scand. J. Plast. Surg., 2: 16, 1968.
- Tumbusch W., Vogel E., Buthiewicz J., Craber C.,
Larson D.,Mitchell E.: Septicemia in bum injury. J. Trauma, 1: 24, 1961.
|