| Annals of the MBC - vol. 3 - n'4 - December 1990
EVOLUTION AND RESULTS OF THE PROPHYLAXIS AND
MANAGEMENT OF INFECTION IN A BURN UNIT, OVER A FOUR-YEAR PERIOD
Herruzo-Cabrera R. *, Lenguas Portero F. **, Martinez-Ratero
S. **, Garcia Torres V. **, Rey Calero J. *
* Preventive Medicine Service, La Paz. Hospital, Madrid,
Spain
** Burn Unit, La Paz. Hospital, Madrid, Spain
SUMMARY. The authors studied
the incidence of mortality and hospital infection (together with the consumption of
antibiotics and financial saving) in a Burn Unit, over a 4-year period, in relation to
various modifications introduced into therapeutical management. Mortality was reduced
after the second year and the incidence of infection was lower every year (in the fourth
year it was 25% that of the first). The aetiology and site of infection also modified:
local bum infection reduced to 25% in the period, with only P. aerugmosa and &
epidermidis retaining an appreciable incidence; sepsis was similar in evolution to
local bum infection; urinary tract infection had a very low incidence in all the period;
other soft tissue infection became predominant in the fourth year, owing to an appreciable
reduction of the more classic infections. The evolution of the consumption of antibiotics
is not related to the infection rate, owing to the great use of third-generation
cephalosporins in the central years of the period. A comparison, after direct
standardization, between the events in the overall period and those in the fourth year
shows that there has been a considerable financial saving (9-28 million pesetas), as a
result of the new therapeutic measures introduced.
Introduction
Infection is one of the most frequent and severe
complications in patients who have ' sustained burns, and particularly so in the case of
those whose burned body surface area exceeds 30% of the total (1, 2), It is also the main
cause of death in these patients after the aspiration syndrome, ranging between 50 and 75%
according to Lutterman and al. (3).
Foremost among the predisposing factors for infection in bum patients are the destruction
of skin and mucosal barriers to micro-organism penetration, the elimination of the normal
resident flora, the loss of antibodies and other proteins into the exudate (which in
itself constitutes an excellent bacteriological culture medium), the reduction of the
fibronectin and complement levels, and the derangement of specific and non-specific cell
mediated immunity, which induces a transient immunosuppression (4-9).
The aetiological agents of infection in bum patients have changed, as in other nosocomial
infections, from a predominance of Gram-positive germs to a predominance of Gram-negatives
(enterobacteria, Pseudomonas, multiresistant enterobacteria) and the presence of
yeasts, as a consequence of the greater selective pressure of antibiotics (1, 10, 11).
Regarding the correct- management of these patients, one should stress the crucial
importance of early debridement and occlusive covering of the burn (12, 13) and other
measures such as perioperatory prophylaxis, local prophylaxis and/or therapy with
antiseptic creams to minimize bacterial colonization (14, 15), selective intestinal
decolonization with non-absorbable drugs so as to control the number and type of
micro-organisms in their greatest reservoir and to prevent the distortions of this flora
caused by various factors such as intestinal stasis, intercurrent antibiotic therapy, etc.
(16, 17, 18), and rhino-oropharyngeal decolonization (19). The purpose of these measures
is to reduce the colonization of these areas and hence the possibility that they may
become the source of contamination and/or infection of other more critical ones, such as
the bums themselves, the respiratory tract (by germs from the pharyngeal contents,
particularly in intubated patients), catheters, etc. (29); a prerequisite to this purpose
is an adequate bacteriological surveillance and monotorization from the moment of
admission into the burn unit, so as to diagnose the infections and study the colonizing
flora and thus make possible an intervention directed at the more pathogenic or resistant
organisms, with the least possibile effect on the more harmless ones.
The purpose of the present communication
is to present our experience in the preventive and therapeutical management of infection
in bum patients, analysing the results over the past four years and discussing the
successive modifications introduced into the therapeutic management.
Material and methods
The population studied comprises all the patients
admitted to the critical area of the Bum Unit at the La Paz Hospital in adrid over the
years 1984-1987. The pertinent data were recorded in a standard chart (Tab. 1) and then
transformed into monthly or three-monthly reports depending on the number of cases. For
the present work, these data have been grouped on a yearly basis.
Name
..........................................…………..
Age Date of admission…………………….
Date of discharge …….
Died (Yes / No)
Depth of bum and % body surface area burned ...............
Cause of bum .. ~ ............................................
Elapsed time between bum and immediate therapy .........
Previous admission in another hospital (Yes / No)
Received antibiotics prior to admission in this bum unit
(Yes / No / Unknown)
Previous / associated disease ..................................
Manipulations
Urinary catheter (dates)
....................................…
Parenteral nutrition (dates) ....................................
Assisted ventilation (dates) ....................................
Surgery (date, type) ........................................…
Other ...............................……………….....
Clinical data
Fever (dates) :
Isolates (micro-organism, date and sample) ............
Therapy
Type of antimicrobial .....................................
Dose per day ................................................
Dates when given ...........................................
Intestinal decolonization (Yes / No)
Immune stimulation (Thymostimulin - Autovaccine)
Plasmapheresis (dates) ................…………….. |
|
Table I Epidemiological
infection surveillance chart for nosocomial infections in the critical area of the Burn
Unit, La Paz Hospital, Madrid |
|
The incidence of
infections was studied in two ways: as cumulative incidence (%) and as incidence density
per patient/month (21).
The antimicrobial drug consumption was assessed in terms of pesetas/antibiotics,
pesetas/treated patient and DDD 100 bed-days (22).
Mortality was divided into "overall" and "non -immediate" mortality,
the latter being defined as that occurring beyond the period of 48 hours after admission;
this allows for inclusion of those patients in whom the presence or absence of therapeutic
effect can be best observed.
For the statistical analysis of the data the Chi-square test and the differences of means
and percentages were applied (21, 23). Some variables along the four years of the study
period were standardized by the direct method (24), using the 1987 population as
reference.
The criteria used for diagnosis of infection were those laid down by Bennett (25) and
Halley (26).
The microbiological analysis of burn, pharyngeal and rectal swabs was carried out at
weekly intervals; that of other specimens (urine, sputum, catheters, etc.) was performed
according to the clinical situation and requirements. The results governed the
prophylactic and therapeutic interventions.
The four years included in the study period differed in some aspects:
- from 1985 onwards, three trained intensive care physicians
were assigned to the Unit;
- in 1985, intestinal decolonization was carried out with
collmycin, 16.5 mg t.i.d., and surgery was performed more often than in 1984;
- in 1986, intestinal decolonization with colimycin was
increased to 33 mg t.i.d. (substituting norfloxacin in the case of bacterial species or
strains with natural resistance, such as Proteus or Serratia), and immunological
stimulation was attempted with pla§mapheresis (7.2%) and thymostimulin (28%). Recourse to
surgery also increased, and chlorhexidine (0.5%) was substituted for silver sulphadiazine
in resistant cases.
Perioperatory prophylaxis was instituted,
with a beta-lactam plus an aminoglycoside, starting one hour before surgery and continuing
for 48 hours; pharyngeal decolonization with hexetidine was performed in all patients
requiring respiratory assistance.
In 1987 the use of thymostimulin was reduced to a minimum, as the drug was not available
over most of the year, and decolonization was performed as explained in Tab. 2. The
frequence of surgery (per patient) was similar to that of the previous year.
Results
The 947 patients forming the study population are
classified in Tab. 3 according to age, percentage of body surface area burned and year.
The percentage distribution is similar for the four years (no significant difference in
the Chi-square test), although in the last two years there is a marked increase in the
number of admissions, particularly in the older age groups.
| A) Perioperatory prophylaxis Cephazoline 2 g + tobramycin 100 mg i.v. 30
minutes before surgery; repeat after six hours.
B) Intestinal decontamination (as long as
manipulations such as i.v. lines, assisted ventilation, bladder catheterization, etc. are
being applied)
Colimycin, 33 mg p.o.. q.i.d. Nistatin, 1
MU p.o., t.i.d.
Erythromycin, 500 mg p.o., t.i.d.
C) Rhinopharyngeal decontamination (as
long as mampulatiow, are being applied)
Chlorhexidine, 0.5% cream, in nares (in
Gram-negative colonization)
Fusicid acid, cream, in nares (in Gram-positive colonisation)
Hexetidine, swabbed onto orodental folds and sprayed onto oropharynx
D) Decontamination of burn and
neighbouring area (until bum is covered)
Chlorhexidine, 0.51Yo cream (rotating
weekly with Silver sulphadiazine, 1%) |
|
Table 2 - Infection
prophylaxis in burn patients |
|
| TABLE 3-1, 1984 |
b.s.a.b.
% |
age |
| < 16
years |
16-64 years |
> 65
years |
TOTAL |
>=60% |
2
1.25% |
5
3.1% |
2
1.25% |
9
6% |
30 -
59% |
3
1.9% |
12
7.5% |
2
1.25% |
17
11.2% |
11 -
29% |
4
25% |
29
18.1% |
4
2.5% |
37
24.5% |
<=10% |
15
9.4% |
70
43.7% |
12
7.5% |
97
64.2% |
TOTAL |
24
15% |
116
72.5% |
20
12.5% |
160
100% |
|
TABLE
3-2, 1985 |
b.s.a.b. |
age |
| <16 years |
16-64 years |
>65 years |
TOTAL |
| >. 60% |
1 |
5 |
1 |
7 |
| |
0.5% |
2.6% |
0.5% |
3. 7 |
| 30- |
3 |
32 |
4 |
39 |
| 59% |
1.6% |
16.7% |
2% |
20.4 |
| 11- |
2 |
30 |
6 |
38 |
| 29% |
1% |
15.7% |
3.1% |
18.9 |
| <=10% |
21 |
72 |
21 |
114 |
| |
11% |
37.7% |
11% |
59.7 |
| TOTAL |
27 |
133 |
31 |
191 |
| |
14.1% |
69.6% |
16.2% |
100 |
|
TABLE
3-3, 1986 |
b.s.a.b. |
age |
| <16 years |
16-64 years |
>65 years |
TOTAL |
| ~:60% |
3 |
9 |
1 |
13 |
| |
1% |
2.9% |
0.3% |
4.2 |
| 30- |
5 |
24 |
2 |
31 |
| 59% |
1.6% |
7.8% |
0.6% |
10.1 |
| H- |
8 |
33 |
8 |
49 |
| 29% |
2.6% |
10.8% |
2.6% |
16% |
| :510% |
20 |
152 |
41 |
213 |
| |
6.5% |
49.7% |
13.4% |
69.6 |
| TOTAL |
36 |
218 |
52 |
306 |
| |
11.8% |
71.2% |
17% |
100 |
|
TABLE
3-4, 1987 |
b.s.a.b. |
age |
| <16 years |
16-64 years |
>65 years |
TOTAL |
| >=60% |
0 |
11 |
4 |
15 |
| |
0% |
3.8% |
1.4% |
5.7 |
| 30- |
2 |
27 |
1 |
30 |
| 59%) |
0.7% |
9.3% |
0.3% |
10.3 |
| 11- |
3 |
34 |
12 |
49 |
| 29% |
1% |
11.7% |
4.1% |
16.9 |
| < 10% |
14 |
155 |
27 |
196 |
| |
4.8% |
5 3.4% |
9.3% |
67.6 |
| TOTAL |
19 |
227 |
44 |
290 |
| |
6.6% |
78.3% |
15.2% |
100 |
|
Table 3 - Distribution of the
studied population (n = 947) by age, percentage of body surface area burned (b.s.a.b.) and
year |
|
VARIABLE
|
YEAR |
| 1984 |
1985 |
1986 |
1987 |
| Absolute mortality |
25 |
22 |
20 |
31 |
| Relative mortality |
16.6% |
11.5% |
6.5% |
10.7% |
| Relative non immediate
mortality |
13.1% |
6.6% |
50% |
9.4% |
| Mean age of dead |
49.4+/-6.3 |
50.9+/-6.3 |
56.1 +/- 5.8 |
58.9+/-4.6 |
| Mean percentage
of body surface area burned in the dead |
43.2+/-6.2 |
51.3+/-6.1 |
38.3+/-7.6 |
46.9+/-5.7 |
| Number of patients with electrical
bums |
4 (2.6%) |
9 (4.7%) |
19 (6.2%) |
23 (7.5%) |
|
Table 4 - Mortality |
|
MANIPULATION
(MEAN %) |
YEAR |
| 1984 |
1985 |
1986 |
1987 |
| Bladder catheter |
15 |
33 |
46.5 |
64 |
| Intravenous fluids |
20 |
56.7 |
62.4 |
35% |
| Parenteral nutrition |
10 |
31.3 |
32.5 |
26 |
| Assisted ventilation |
n.d. |
4.5 |
10.8 |
37 |
| Surgery (N. of interventions/100
patients/month) |
30 |
67 |
101 |
99 |
|
Table 5 - Manipulations |
|
STUDIED VARIABLES |
YEAR |
| 1984 |
1985 |
1986 |
1987 |
| Mean number of patients/month with
admission ~24h |
12 |
18 |
20 |
17 |
| Cumulative incidence of infection
(%) |
41.3 |
36.4 |
24.2 |
24 |
| Incidence density of infection
(patients/month) |
1.85 |
1.61 |
0.99 |
0.51 |
| Mean duration of admission/month for
infected patients |
19.6 |
17.9 |
19.1 |
19.9 |
| Mean duration of admission/month for
nominfected patients |
7.7 |
7.8 |
8.8 |
9.9 |
| Incidence density
for burn Infection |
| * TOTAL |
1.04 |
0.831 |
0:38 |
0.116 |
| * P. aeruginosa |
0.355 |
0.392 |
0.142 |
0.1 |
| • Enterobacteria |
0.646 |
0.435 |
0.157 |
0 |
| • Staphylococcus: |
|
|
|
|
| - Total |
0.525 |
0.176 |
0.079 |
0.014 |
| -S. aureus |
0.525 |
0.145 |
0.079 |
0 |
| - S. epidermidis |
0 |
0.033 |
0 |
0.014 |
| • Anaerobes |
0.148 |
0.176 |
0.016 |
0 |
| • Fungi |
0.031 |
0 |
0 |
0.014 |
| • Other micro-organisms |
0.18 |
0.226 |
0.132 |
0.014 |
| Incidence density for sepsis |
|
|
|
|
| * TOTAL |
0.659 |
0.614 |
0.17 |
0.116 |
| * P. aeruginosa |
0.061 |
0.165 |
0 |
0.043 |
| • Enterobacteria |
0.182 |
0.148 |
0 |
0 |
| • Staphylococcus: |
|
|
|
|
- Total
|
0.326 |
0.29 |
0.111 |
0.028 |
-S. aureus
|
0.239 |
0.072 |
0.016 |
0.014 |
- S. epidermidis
|
0.086 |
0.217 |
0.095 |
0.014 |
| • Anaerobes |
0.024 |
0 |
0 |
0.014 |
| • Fungi |
0 |
0.035 |
0.063 |
0 |
| • Other micro-organisms |
0.106 |
0.064 |
0.047 |
0.029 |
| Incidence densityfor
other soft tissue infection |
| * TOTAL |
1.062 |
0.18 |
0.27 |
0.173 |
| * P. aeruginosa |
0 |
0 |
0.016 |
0.173 |
| • Enterobacteria |
0 |
0.015 |
0.016 |
0.029 |
| • Staphylococcus: |
|
|
|
|
- Total
|
0.062 |
0.09 |
0.126 |
0.058 |
- S. aureus
|
0.062 |
0.03 |
0.063 |
0 |
- S. epidermidis
|
0 |
0.06 |
0.063 |
0.058 |
| • Anaerobes |
0 |
0.03 |
0 |
0 |
| • Fungi |
0.031 |
0 |
0.03 |
0.047 |
| • Other micro-organisms |
0 |
0.015 |
0.063 |
0.043 |
| Incidence density
for urinary tract infection |
| * TOTAL |
0.185 |
0.033 |
0.11 |
0.043 |
| * P. aeruginosa |
0 |
0 |
0.031 |
0.014 |
| • Enterobacteria |
0.031 |
0.033 |
0.064 |
0.029 |
| • Staphylococcus: |
|
|
|
|
- Total
|
0 |
0 |
0.016 |
0 |
- S. aureus
|
0 |
0 |
0.016 |
0 |
- S. epidermidis
|
0 |
0 |
0 |
0 |
| • Anacrobes |
0 |
0 |
0 |
0 |
| • Fungi |
0.031 |
0 |
0 |
0 |
| • Other micro-organisms |
0.092 |
0 |
0.031 |
0 |
|
Table 6 - Incidence, aetiology and site of infection |
|
| INDEX STUDIED/1987 |
1984 |
1985 |
1986 |
1. Excess admissions due to
infection
(inf. = infection) |
1328 |
1144 |
471 |
| (+ 101 inf.) |
(+ 114 inf.) |
(+ 46 inf.) |
| 2. Admission costs, Ptas, due to infection
(mill. = 1000000, Ptas = pesetas) |
33.2 mill. |
28.6 mill. |
11.8 mill. |
| 3. Antimicrobial costs, Ptas |
1.74 mill. |
2.72 mill. |
4.37 mill. |
| 4. Saved excess admissions in infected patients
(earlier discharge) |
- 60 |
- 144 |
- 48 |
| 5. Admission costs, Ptas, due to 4. |
1.5 mill. |
3.6 mill |
1.2 mill |
| 6. Saved excess admissions in non infected
patients (earlier discharge) |
- 185 |
7.6 mill. |
5 mill. |
| 7. Admission costs, Ptas, due to 6. |
- 4.6 mill. |
7.6 mill. |
5 mill. |
| Total difference in expenditures: (2 + 3 - 5 -
7) |
+ 27.9 mill. |
+ 19.1 mill. |
+ 9 mill. |
|
Table 7 Economical repercussions
of infection |
|
The mortality data
are collected in Tab. 4, which shows that the two intermediate years differ significantly
form the first (but not from the fourth) in non-immediate mortality. There were no
significant differences in age and burned body surface area percentage among the fatal
cases over the four years. In 1987 the number of patients with electrical burns was
greater than in the preceding years, although the ditTerence is only significant for the
comparison with 1984, due to the small size of the sample. Tab. 5 summarizes the
manipulations performed on the patients. There was an increase in time for most
manipulations, which was greatest for assisted ventilation and blader catheterization.
Surgical interventions also increased 100% from 1984 1986-1987. Tab. 6 shows the
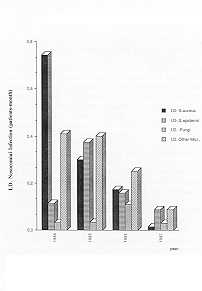
incidence, aetiology and site of infections. These data are graphically summarized in
Figs. 1, 2 and 3. A striking observation is the decline of infection, both when considered
as cumulative incidence and as incidence density, during the last two years, and even more
so in 1987, when the infections per patient per month represent only one quarter of the
figure for 1984. Furthermore, the most frequent infection in this last year (in spite of
the decline as compared to the previous ones) is that in "other soft tissues"
(with non-significant differences between 1984-87), due to the even more drastic reduction
of infections of other sites (particularly bum P < 0.001). As to the aetiology of
infections, there was a very marked fall of all organisms in burn infections (p <
0.001), and only Pseudomonas retain an appreciable incidence (although this is only
25% of that during the first two years). Enterobacteria, the main cause of burn
infections, disappeared in 1987. There has also been an inversion of the relative
frequencies of both types of staphylococcl (S. aureus and S. epidermidis), as
S. aureus, which was more frequent in previous years, disappeared, and only S. epidermidis
had a small representation in the last year of the study.
The cases of sepsis indicate an overall reduction to one sixth of the initial incidence (p
< 0.001); the main causative agent is now Pseudomonas for even though its
incidence is lower than in the first two years it has become predominant due to the
greater reduction (p < 0.001) of the other organisms (except anaerobes and fungi:
non-significant difference).
In 1984, sepsis due to Gram-positive cocci was caused mainly by S. aureus. Over the
following two years S. epidermidis predominated, in spite of the overall reduction
of this type of infection, and in 1987 both types of staphylococci were isolated with
similar low frequency.
Infections of the soft tissues were those which benefited least from the therapeutic
measures introduced in 1987, with a non-significant reduction, although S. aureus was
no longer represented as an aetiological agent and there was a slight increase in the
incidence of Gram-negative rods.
Infection of the urinary tract also showed a reduction (p < 0.001 between 1984-87),
while other infections hardly need to be mentioned; foremost among these are the
infections of the respiratory tract.
When calculating the overall germ-specific incidence of infection, regardless of site,
there is a clear decline for all micro-organisms in 1987, as compared to previous years:
330-1340% for enterobacteria, 10-1230% for anaerobes, 1240-5300% for S. aureus, 10-370%
for fungi, 0-240% for Pseudomonas, 30-430% for S. epidermidis, and 300-470%
for other organisms (mainly S. faecalis).
Consumption of antibiotics, which is represented in Figs. 4, 5 and 6, declines in parallel
to the incidence of infection with the exception of years 1985-86, where consumption was
high due to increased use of third-generation cephalosporins and aminoglycosides.
Finally, Tab. 7 compares several indices of the four years, standardized with 1987 as the
reference year. This comparison shows a "saving" of 46-114 infections and of
9-28 million pesetas (admissions plus antimicrobial drugs) as an effect of the
introduction of the new therapeutic measures.
Discussion
The foremost and most remarkable finding of this
retrospective review is the dramatic decrease in the number of infections achieved during
the last two years of the study period, when double prophylaxis (intestinal and
perioperatory) was applied, and most particularly in 1987, when perioperatory prophylaxis
was reduced to a valid minimum (two doses) and intestinal prophylaxis was carried out with
three drugs and associated to local action on the pharynx.
These procedures achieved a striking reduction of all infecting micro-organisms, and the
reduction is rather less striking only in the case of infections of other tissues due to Pseudomonas,
in spite of the particular attention paid to the protective measures (27).
The great impact that prophylaxis achieved on the incidence of infections demonstrates the
endogenous origin of the immense majority of these complications in this type of patient
(28); only in a few cases of nonfermenting bacilli was an endogenous infection suspected,
although we were unable to demonstrate the mechanism of transmission (hands of nursing
staff, inert carriers, etc.).
We also had some failures in intestinal decolonization, in spite of the established
prophylaxis, which were caused in most cases by multiresistant
 |
 |
| Fig. 1 - Distribution
of Hospital Infection (measured in incidence density). |
Fig. 2 -
Aetiology of Hospital Infection (incidence in density of incidence). |
 |
 |
| Fig. 3 - Aetiology
of Hospital Infection (continuation) (incidence i density of incidence). |
Fig. 4
- Density of infection incidence in relation to antibiotic use (expressed in DDD per 100
Bed-days). |
|
Pseudomonas.
This may be explained by the fact that
the dose of colimycin used for prophylaxis was too low for this organism, although it was
fully effective for controlling enterobacteria. For this reason, in 1988 we introduced
prophylaxis with colimycin at a dose of 600-800 ing/day (18), using oral norfloxacin or
tobramycin if bacteria were selected which are naturally resistant to colimycin, such as Proteus
or Serratia.
As shown in Fig. 3, the incidence of fungal infections increased (non-significantly)
in 1986. This was a consequence of the increased consumption of antibiotics, mainly
third-generation cephalosporins. The incidence of fungi as aetiological agents again
diminished in 1987, for two reasons: reduction of the use of selected antibiotics (for
instance, two instead of five doses for perioperatory prophylaxis) and association of an
antifungal agent (Nistatin) for decolonization of the intestinal reservoir, although the
dose we used was lower than that suggested by Stovtenbeek (17) and Clasener (18); even so,
it was highly effective in preventing infection by these organisms. In 1988 the dose of
Nistatin was increased when Candida was isolated from stools, and so far all detected
colonizations have been eradicated.
Staphylococcus epidermidis infections are mainly associated to intravenous fluids
and catheters, and increase in parallel with these manipulations. The greater attention
materials has led infections and aureus has develonment paid to these manoeuvres
and to a reduction in the number of to a change in their aetiology, where S. replaced S. epidermidis,
but the of such infection must be further reduced, an aim we hope to achieve through
the new measures (local application of 0.5% chlorhexidine cream onto the area of insertion
of catheter: the initial results of this procedure have been optimal).
 |
 |
| Fig. 5 -
Antibiotic use. Description. |
Fig. 6 -
Betalactarn. Antibiotic use. |
|
In spite of the large proportion of
patients requiring assisted ventilation (33% in 1987), the incidence of respiratory
infections was minimal; we believe this finding to decolonization with demonstrated in a
study intensive care unit (19).
The striking reduction of the infections cannot be explained solely by the greater
recourse to surgery. The number of surgical interventions increased over the first three
years of the study period, but in the fourth year, with a similar proportion of surgical
interventions per patient, there was a reduction of the infections to half the number of
the previous year. Furthermore, the decline of infections achieved between 1985 and 1986
was much greater than the increase in the frequency of surgery, which was similar to that
from 1984 to 1985. These observations underline the importance of global decolonization in
the early management of the bum patient.
The increased mortality in 1987 as compared to the two preceding years, although
non-significant, might be due to the greater age of the patients who died (2-9 years), to
the worse state on admission (increased frequency of aspiration syndrome) and/or to
multisystem failure, as suggested by the increase be related to pharyngeal hexitidine, as
already carried out in a different (3.4 to 8.2 times) of the proportion of patients
requiring assisted ventilation, and to the greater number of patients with electrical bums
(4-14).
With regard to antimicrobial drug consumption, in 1987 there was a reduction in both the
overall consumption and the consumption per patient; there was also a change in
antimicrobial usage, from the predominantly therapeutic usage during the first years of
the study to the mainly prophylactic usage in 1987.
The increased expenditure on antimicrobials observed in 1985-86 was primarily due to the
use of first- and third-generation cephalosporins (Figs. 5 and 6) which, in the case of
perioperatory prophylaxis (first-generation cephalosporins), might imply a link-up with
that of a second intervention, if this took place three or four days after the previous
one.
This problem was obviated in 1987, when only two doses were given (before and after
surgery), so that even though a greater number of perioperatory prophylaxis regimens were
given, both the overall usage of antimicrobials and the selection of resistant strains in
the intestine decreased.
Finally, when translating the balance of the infection rates in the unit into
"pesetas", a considerable saving effect becomes evident (9 to 29 million
pesetas, according to the various years), together with a further saving that is not
easily amenable to economical measurements, i.e. that of suffering, of sequelae and also
of mortality, which would have been the consequence of the 46 to 101 infections that did
not occur.
We therefore stress the great interest of the global prophylactic regime used (Tab. 2),
together with the two modifications described in the text, for reducing, together with
surgery, the number of infections of all origins in patients sustaining bum injuries.
RÉSUMÉ. Les Auteurs ont
étudié la fréquence de la mortalité et de l'infection hospitalière (et en même temps
la consommation des antibiotiques et l'épargne économique) chez une Unité de Brûlures,
pendant une période de 4 ans, par rapport aux diverses modifications introduites dans la
gestion thérapeutique. La mortalité était réduite après le deuxième an, et la
fréquence de l'infection était plus basse tous les ans (au quatrième an elle était 25%
par rapport au premier an). Il y a eu aussi des modifications pour ce qui concerne
l'étiologie et le site de l'infection: l'infection locale causée par la brûlure a
diminué à 25% dans la période, et seulement P. aeruginosa et S. epidermis ont
maintenu une fréquence sensible; les infections généralisées ont eu une évolution
semblable à celle des infections locales des brûlures; l'infection aux voies urinaires a
eu une fréquence très basse pendant toute la période; les autres infections du tissu
mou sont devenues prédominantes au quatrième an à cause d'une réduction des infections
plus classiques. L'évolution de la consommation des antibiotiques n'est pas corrélée au
taux d'infection, à cause de l'emploi très large des céphalosporines de la troisième
génération pendant les années centrales de la période; une comparaison, après la
standardisation directe, entre les évènements pendant la période complessive et ceux de
l'an final indique une épargne économique considérable (9-28 millions de pesetas),
comme conséquence de l'introduction des nouvelles techniques thérapeutiques.
BIBLIOGRAPHY
- McManus W.F., Goodwins CW., Manson A.D., Pruitt
B.A.: Bum wound infection. Journal of Trauma: 753-756, 1981.
- Yurt R.W., Shires G.T.: Bums. In: Mandell G.L.,
Douglas R.G. and Bennett J.E., Eds., "Principles and practices of infectious
diseases", Second ed., 628-631, New York, 1985.
- Lutterman A., Dacso C.C., Curreri P.W.: Infections
in bum patients. American Journal of Medicine, 81 (suppl.): 45-52, 1986.
- Gelfand J.A.: Infections in bum patients: A paradigm
for cutaneous infection in the patient at risk. American Journal of Medicine, 76 (Suppl.):
158-163, 1989.
- Alexander C.L., Ogle C.K., Stinnett J.D., McMillan
B.G.: A sequential prospective analysis of immunologic abnormalities and infection
following severe thermal injury. Annals of Surgery: 809-816, 1978.
- Bjornson A.B., Alterneier W.A., Bjornson H.S.:
Complement, opsonin and the immune response to bacterial infection in burned patients.
Annals of Surgery, 191: 323-329, 1980.
- McCabe W.P, Rebuck J.W., Kelly A.P., Ditmars D.M.:
Leukocyte response as a monitor of immunodepression in bum patients. Archives of Surgery,
106: 155-159, 1973.
- Grogan J.B.: Suppressed in vitro chernotaxis of burn
neutrophil. Journal of Trauma, 16: 985-988, 1976.
- Warden J.D., Mason A.D., Pruitt B.A.: Evaluation of
leukocyte chernotaxis in vitro in thermally injury patients. Journal of Clinical
Investigation, 54: 1001-1004, 1974.
- McMillan B.G., Holder F.A., Alexander J.V.:
Infections of bum wounds. In: Bennett J.V. and Brachman P.S., Eds., oHospital
Infections>>, 465-482, Seconded., Little Brown, Boston, 1986.
- Herruzo Cabrera R., Garcia Caballero J., Lenguas F.,
Pintado R., Garcia Torres V., Rey Calero J.: Estudio epidemiol6gico de la infecei6n
hospitalaria en un centro de quemados durante los ahos 1984-85: Comunicaci6n XI
International Congress of Preventive and Social Medicine, Madrid, 1986.
- Demling R.H.: Improved survival after massive bums.
Journal of Trauma, 23: 179-184, 1983.
- Engnav L.H., Heimbach D.M., Reus J.L., Haman T.J.,
Marvin S.A.: Early excision and grafting versus nonoperative treatment of bum of
indeterminate depth: a randomized prospective study. Journal of Trauma, 23: 1001-1004,
1983.
- Herruzo Cabrera R., Garcia Torres V., Rey Calero J.:
Estudio de la actividad bacteriostàtica y bactericida de 7 cremas antisépticas y
evaluaciôn de su poder de penetraciôn mediante un modelo in vitro. Comurlicaciàn al Il
Congresso SEIMC, Mallorca, 1986.
- Herruzo Cabrera R., Pintado Otero R., Rey Calero J.,
Garcia Torres V.: Complicaciones infecciosas en enfermos quemados. Revista Iberoamericana
de Cirugia Pldstica, 14: 257-264, 1988.
- Van der Vaaij D.: The colonization resistance of the
digestive tract in experimental animals and its consequences for infection prevention,
acquisition of new bacteria and the prevention of spread of bacteria between cage mates.
in: Van der Vaaij D., Verhoef J., Eds., "New criteria for antimicrobial therapy:
maintenance of tract colonization resistance", 43-53, Excerpta M6dica, Amsterdam,
1979.
- Stovtenbeek C.P., Van Sacne H.K.F., Miranda D.R.,
Zandstra D.F.: The effect of selective decontamination of the digestive tract on
colonization and infection rate in multiple trauma patients. Intensive Care Medicine, 10:
185-192, 1989.
- Clasener H.A.L., Vollaard, Van Saene H.K.F.:
Longterm prophylaxis of infection by selective decontamination in leukopenia and in
mechanical ventilation. Review of Infectious Diseases, 2: 295-238, 1987.
- Rodriguez Artalejo F., Herruzo Cabrera R., Garcia
Caballero J., Rey Calero J.: Methodologic approaches for the study of pneumonias in
intensive care units. XI Congress of Preventive and Social Medicine, Madrid, 1986.
- Herruzo Cabrera R., Garcia Torres V., Rey Calerc,
J.: Control de la Infecci6n en Quemados. Revista Iberoamerjcan~ Cirugia Pldstica, 14:
189-196, 1988.
- Rothman K.J.: in "Epidemiologia Modema",
Diaz de Santos, Ed., 29-41, Madrid, 1987.
- Kennedy S.L., Forbes M.B., Bann C.: Antibiotic use
in U i S. hospitals in 198 1. American Journal of Hospital Pharmacy, 40: 797-801, 1983.
- Carraco J.L.: "El m6todo estadistico en la
investigaci6n m6dica", 167-174, Karpos, Madrid, 1986.
- Lilienfeld A.M., Lilienfeld D.E.: "Fundamentos
de Epidemiologia", 66-68, Fondo Educativo Interamericano, Mexico, 1983.
- Bennett J.V., Brachman P.S., Eds.: "Hospital
Infections", 335-354, Little Brown, Boston, 1979.
- Halley R.W.: "Managing hospital infection
control for cost-effectiveness", American Hospital Publishing, AHA, 1986.
- Palmer M.B.: "Infection Control. A policy and
procedure manual", W.B. Saunders, London, 1984.
- Bennett J.V., Brachman P.S., Eds.: "Hospital
infection", 465-487, Little Brown, Boston, 1986.
|