Annals of the MBC - vol. 4 - n' 1 -
March 1991
MODIFICATIONS OF
COAGULATION IN THE BURN PATIENT,
Garcia Torres V., Jimenez M.C., Garcia Salvatierra B.,
Rivera M.J., Guemes Gordo F.
Burns Unit, Plastic and Reconstruction Department, La Paz
Hospital, Madrid, Spain
SUMMARY. Twenty-six patients admitted to our
Hospital with bums of different extent, type and degree, were studied. Coagulation studies
were performed on all of them in order to detect the possibility of hypercoagulation. The
results of this test were compared to another performed on the same patient once he/she
was discharged from hospital. Our findings support the hypercoagulation thesis expressed
in terms of platelet activation, higher fibrinogen levels and lack of fibrinolytic
response, jointly with a significant reduction in AT 111. We suggest heparin prophylaxis
on an individual basis, in order to prevent the appearance of thromboembolic phenomena in
these patients.
Introduction
Thromboembolic disease, with its first manifestation, deep
venous thrombosis (DVT) and its severe complication, pulmonary- embolism (PE), is a common
finding in severely burned patients (1, 2).
Significant fibrinogen and platelet consumption, and haemorrhage due to disseminated
intravascular coagulation (DIC), have also been recorded in the literature linked to
thermal injury (3, 4).
These findings have led to considering heparin therapy in the severely burned patient.
This approach has gained much acceptance in other clinical aspects of the burned patient
(5), but heparin effectiveness in the prevention of thromboembolic disease is still
uncertain.
A coagulation protocol has been applied in our study in order to explore the different
aspects and to assess analytically whether these patients present signs of
hypercoagulation within the first 72 of their base pathologic condition.
No previous patient selection was performed since another of our objectives was to
determine whether hypercoagulation states were linked to the extent of the bum.
Once patients were dismissed from hospital and thus considered clinically cured, they
underwent the same coagulation studies as on admission. This second study was considered
to represent the basal values of each patient.
The results obtained in each parameter or set of parameters have been assessed in relation
to the basal results obtained for the whole of the patient population. DIC was not
observed among our cases as a thrombotic manifestation. On the other hand, enough
information was gathered to state that there exists a thromboembolic tendency in our group
of burned patients, which is unrelated to the extent of the bum, and presenting as one of
the most relevant changes a decrease in antithrombin Ill, an essential coagulation
inhibitor. At III decrease in itself predisposes towards thrombosis in any subject.
On the basis of our results we propose individual prophylaxis in these patients (5) in
order to prevent thromboembolic disease more effectively.
Material and methods
Twenty-six patients (17 male and 9 female, aged 9 to 89
years) admitted to the Bum Unit at our hospital participated in our study. All patients
underwent coagulation tests within ihe first 72 hours of admission. Similar tests were
performed on patient discharge and were considered the patient's basal coagulation
profile. The blood obtained from venipuncture is divided into the following tubes: 2
plastic tubes with 1/9 sodium citrate; I tube prepared with EDTA for haematimetry and
platelet tests; I tube containing fibrinolysis inhibitors for FDP and I tube containing
platelet activation inhibitors for pF4 and 0 -thromboglobulin.
The tests performed may be divided into two groups:
Overall coagulation tests:
Prothrombin activity
Cephalin time
Fibrinogen
Platelet number
Tests geared to exclude the possibility of DIC and to determine ibnno ytic system c anges:
Fibrinogen degradation products (FDP)
Euglobulin lysis using von Kaulla's method
Fibrinolytic system estimation through Astrup's plates (6)
Ethanol test'
Fibrin monomer determination
Thromboelastograms were performed to determine the structural hypercoagulation status of
the blood.
All haemostasis techniques were performed according to Caen et al (7).
Antithrombin 111 was measured using chromogenic susbtrate methods (8).
P-thromboglobulin and platelet factor 4, the increase of which in blood -is an indication
of the platelet activation index, were measured (9). The former was measured by RIA using
a commercial kit from Radiochemical Centre, Amersham. Both the technique and sample
preparation have been described previously (10, 11). The latter factor (pF-4) was also
measured by RIA using the commercial kit from Abbott Laboratories, Diagnostics Division
(12).
The coagulation tests were supplemented with haematocrit and haemoglobin measurements, two
parameters that permitted the assessment of haemoconcentration.
All techniques were performed on all patients on both measurements and compared to each
other.
The statistical analysis of the results was done using Student's t test and variance
analysis.
Results
Tab. 1 shows the types of bums suffered by the 26 patients
in our study. Tabs. 2 and 3 show the degree and extent of the burns.
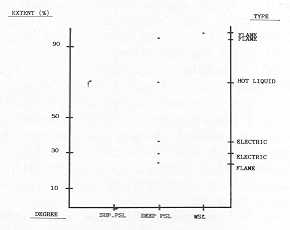
Six of the patients died during the first hours of hospital stay. Fig. 1 shows the main
features of the bums suffered by these patients.
The tests generally performed after hospital discharge were not done on the 6 deceased
patients for obvious reasons, and on 4 other patients who did not return for follow-up due
to geographical reasons.
The following results were obtained in the overall coagulation tests.
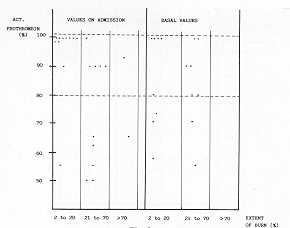
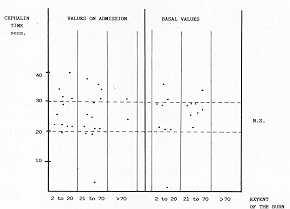
Both prothrombin activity (Fig. 2) and cephalin time (Fig. 3) fell within normal or
slightly longer times, which was interpreted to reflect the consumption of some
coagulation factors. Return to normal levels was not achieved in all patients by hospital
discharge, especially the vitamin K-dependent factors measured through prothrombin
activity. The difference observed was not significant.
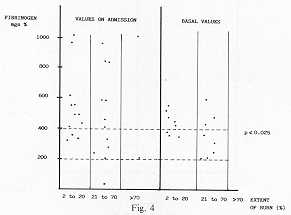
Fig. 4 shows the fibrinogen level presented by our patients. A marked increase can be seen
in 17 patients, which was statistically significant when compared to their own basal
levels (p< 0.025). It must be noted that the fibrinogen level did not relate to the
extent of the bum.
 |
 |
| Fig. I Characteristics
of the bums ofsix deceased patients |
Fig. 2 Prothrombin
activity statistically: N.S. The space between the horizontal lines corresponds to the
area of normal values |
 |
 |
| Fig. 3 Cephalin
time The space between the horizontal lines corresponds to the area of normal values |
Fig. 4 Fibrinogen.
Levels The space between the horizontal lines corresponds to the area of normal values |
|
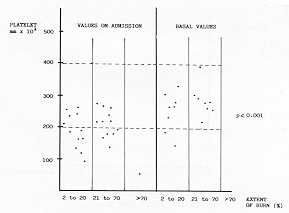
Fig. 5 shows the platelet count in whole
blood. There is a statistically significant (p<0.001) tendency towards thromboeytopenia
observed on admission. Despite this finding, there were only 2 thrombopenic patients with
levels under 100,000 platelets and, overall, this slight decrease in the platelet number
does not seem to account for any disseminated intravascular coagulation.
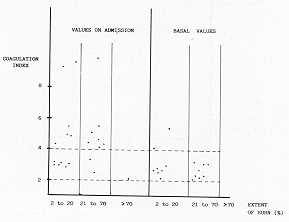
Thromboelastography was used in order to measure the possibility of structural
hypercoagulation of the blood. The set of parameters measured through the
thromboelastogram is reflected in the so-called coagulability index, obtained after using
a previously set formula. Normal values for this index range between 2 and 4. As can be
seen in Figure 6, 13 of our patients showed marked hypercoagulation, that is to say, blood
coagulation measured in overall terms was increased. This hypercoagulation state returned
to normal limits in all patients except two, whose extremely high- coagulation index on
admission was returning to normal but had not reached that limit yet.
Once hypercoagulation was verified through these generic methods, we decided to apply more
specific techniques that would help us assess the reasons for the hypercoagulation state.
Euglobulin lysis time was determined in order to determine whether the lytic capacity,
which is capable of reacting to fibrin formation, was increased in our patients' plasma.
All euglobulin lys1s times fell within normal limits, and no significant increases were
observed.
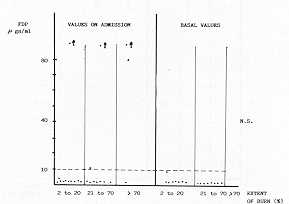
FDPs, which were increased in cases of DIC and/or reactional fibrinolysis, were increased
in 4 of our patients, who on the other hand did not present any other signs in favour of
DIC (Fig. 7). The results obtained were not statistically significant. Onceagain, as in
previous results, there was no relationship between FDP increase and the extent of the
bum.
Two techniques having similar significance and different specificity were used to verify
the presence of fibrin monomers in circulating blood. As shown in Table 4, the fibrin
monomer method, which is more specific, was positive in half of our patients, remaining so
for a long time in a patient with bums over 60% of his body surface.
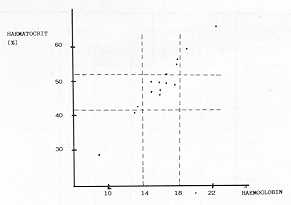
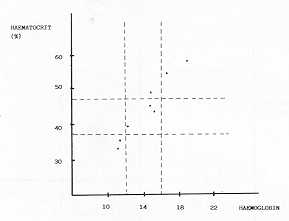
The haematocrit/haemoglobin ratio is represented in Fig. 8 in the case of males and Fig. 9
in the case of females. Eight patients showing haernoconcentration had returned to normal
levels by the time basal tests were performed.
 |
 |
| Fig. 5 Platelet
number in whole blood The space between the horizontal lines corresponds to the area of
normal values |
Fig. 6 Thromboelastogram
coagulation index The space between the horizontal lines corresponds to the area of normal
values |
 |
 |
| Fig. 7 Fibrinogen
degradation products Normal: up to 10 ~' gs/ml |
Fig. 9 Ht/Hb
ratio in female patients |
|
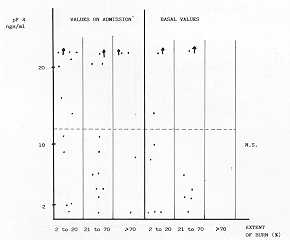
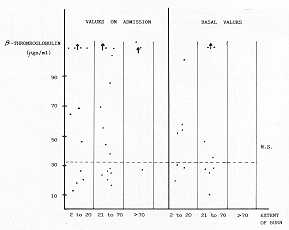
Platelet factor 4 assay and 0-thromboglobulin assay were used to assess the presence of
activated platelets in circulating blood. Both platelet factors were increased in
circulating blood when platelets became activated for any reason.
Both platelet factor 4 and P-thromboglobulin were increased in 50% of our patients, but
without statistical significance (Fig. 11). Also in this case there -was no significance
with the extent of the bum. The values of some of our patients had not returned to normal
during the control study.
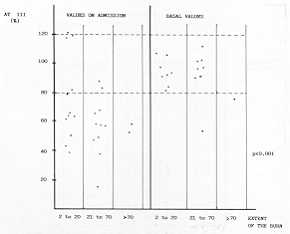
Finally, antithrombin 111, the most important coagulation inhibitor, was measured. Lower
than normal levels increased the risk of thrombosis. Nineteen of our patients showed (Fig.
12) a ,statistically significant decrease in AT III (p<0.001), which had been corrected
by the time the basal tests were performed.
 |
 |
| Fig. 8 Ht/Hb
ratio in male patients |
Fig. 10 Platelet
factor 4 Normal: up to 12 ki gs/ml |
 |
 |
| Fig.11 Normal:
up to 32 lL gs/ml |
Fig. 12 Antithrombifi
III The space between the horizontal lines corresponds to the area of normal values |
|
Discussion
The presence of structural hypercoagulation measured as the coagulation Index through
thromboelastography was evident in our patients. However, such findings do not correlate
with a state of disseminated intravascular coagulation, since there is neither fibrinogen
nor platelet reduction nor FDP increase, which when combined provide the diagnosis of DIC.
Our results show increased fibrinogen levels from the onset of the bum. Since this protein
belongs to the group of the so-called acute stage reacting proteins, its increase may be
considered non-specific and as such does not indicate a hypercoagulation state, although
contributing to it.
Such indirect cooperation of fibrinogen to coagulation is supported by other factors such
as normal or slightly increased prothrombin activity and normal cephalin time, suggesting
an activation of the coagulation chain from thromboplastic substances released from the
burned surface (13, 14).
We did not observe a significant increase in FDPs, contrary to what is commonly reported
in the literature (15, 16, 17), and this relates to a non-increase in plasma fibrinolytic
capacity shown by our patients. This lack of vascular fibrinolytic response may lead to an
accumulation of activated coagulation products over the blood vessel surface.
Likewise, at the onset of the bum no marked change in the platelet number was observed,
and only two patients presented clinically significant thrombopenia. Also, the Ht/Hb ratio
does not suggest a relevant consumption and/or important haemolysis.
Nevertheless, the presence of circulating fibrin monomers suggesting a thromboembolic
tendency in our burned patients was not unusual.
We would like to point out two important findings in our study. First, activated platelets
circulating in the blood stream were a common finding, favouring thrombus formation in
areas of venous stasis or microcirculation.
Secondly, there was a significant decrease in the most important coagulation inhibitor, AT
111. These findings may have two interpretations:
- The factor was consumed in an attempt to control the
activated coagulation factors.
- It may also be related to changes in liver protein
production during the acute stage of the bum. It seems that liver production of acute
stage proteins in the burned patient increases at the expense of other proteins. It has
been suggested that there is an aminoacid shunt from some proteins to others. Some protein
levels therefore increase while others decrease.
Whatever the mechanism may be, the fact
that AT Ill is reduced definitely contributes to the appearance of thrombotic phenomena in
the burned patient.
We may conclude by saying that the high percentage of DVT observed in hospitalized burned
patients, with or without episodic PE, is supported, from a coagulation perspective, by
the following data:
- fibrinogen level increase
- plasma fibrinolytic capacity reduction
- platelet activation
- plasma AT 111 reduction
- that in our group of patients, such changes were not
related to bum extent
- that our patients did not present signs of DIC.
All these findings strongly suggest that
heparin prophylaxis, despite its controversial use, should be undertaken on all burned
patients, regardless of the extent of the bums, especially if they fall within the A-AB
category (5, 18, 19).
We feel that it is important to treat the burned patient also by providing him/her with
plasma therapy and supplying the lost AT Ill, along with individual doses of heparin (20),
in order to provide efficient control of one of the more severe complications in the
burned patient, i.e. thromboembolic phenomena.
| TYPE OF BURN |
NUMBER OF
PATIENTS |
| ELECTRIC |
8 |
| FIRE |
2 |
| FLAME |
10 |
| EXPLOSION |
2 |
| GAS EXPLOSION |
1 |
| HOT LIQUID |
1 |
| CHEMICAL |
1 |
| DEGLOVING ABRASION |
I |
|
| Tab. I |
|
| DEGREE |
NUMBER OF
PATIENTS |
| SUPERFICIAL PARTIAL |
- |
| SKIN LOSS |
2 |
| DEEP PARTIAL |
- |
| SKIN LOSS |
15 |
| WHOLE SKIN LOSS |
9 |
|
| Tab. 2 |
|
| EXTENT (%I |
NUMBER OF
PATIENTS |
2 to
20 % |
10 |
21 to
50 % |
9 |
50 to
60 % |
3 |
| > 60% |
4 |
|
Tab. 3 |
|
| |
ETHANOL |
FIBRIN
MONOMERS |
| |
NEGATIVE |
POSITIVE |
NEGATIVE
|
POSITIVE |
| VALUES ON |
|
|
|
|
| ADMISSION |
21 |
4 |
12 |
13 |
| BASAL |
16 |
- |
15 |
1 |
| VALUES |
|
|
|
|
|
| Tab. 4 |
|
RESUME Les Auteurs ont kudi6
26 patients hospitalis6s chez leur Unit6 de Br-616s qui pr6sentaient des brillures
d'extension, de type et d degr6 variables. Ils ont effectu6 une recherche chez ces
patients pour d6tecter la possibilit6 de I'hypercoagulation. Les r6sultats de cette 6preuv
ont R6 compar6s avec les r6sultats d'une seconde 6preuve ex6cut6e sur le rn~me patient au
moment de la sortie de 116pital. Lanalyse de ce r6sultats confirme la th6se de
I'hypercoagulation exprim6e en termes de I'activation des plaquettes, des niveaux plus
6lev6s du fibrinog6ne e de Fabsence de la r6ponse fibrinolytique, avec une r6duction
significative de I'antithrombine Ill. Les Auteurs proposent 1'emploi de I prophylaxie
h6parinique sur base individuelle pour pr6venir I'apparition des ph6nom&nes
thromboemboliques chez ces patients.
|