| Annals of the MBC - vol. 4 - n' 2 - June 1991
EARLY PREDICTION OF ADULT RESPIRATORY
DISTRESS SYNDROME BY THE STATE OF LEUKOCYTE ADHESIVENESS/AGGREGATION
Pried M., Ben-Hur N., Weiss D. *
Department of Plastic and Maxillofacial
Surgery, Shaare Zedek Medical Center, Jerusalem, Israel
* Department of Radiology, Hadassah Medical Center, Ein-Kerem, Jerusalem, Israel
SUMMARY. The case is described
of a patient with 90% BSA burns who 60 hours post-burn developed acute adult respiratory
distress syndrome (ARDS) and eventually died. A very high level of white blood cell
aggregates was observed soon after admission, reflecting a state of pulmonary
leukoaggregates which are a pathophysiological component of ARDS. The early detection of
impending deterioration in based on the state of leukocyte adhesiveness/aggregation in the
peripheral blood is useful for the assessment of the pulmonary status of severely burned
patients. This is the first. case report in which the subsequent development of ARDS was
predicted before this possibility was suggested by clinical, roentgenological and
biochemical evidence.
A 19-year-old man who suffereed a 90% 2nd-
and 3rd-degree body surface area burn injury developed the acute adult respiratory
distress syndrome (ARDS) 60 hours post-injury. During the laboratory evaluation of the
patient, froM. the time of his admission, his blood was examined sequentially by the
leukergy test which determines the extent of leukocyte adhesiveness and aggregation in the
peripheral blood. A very high level of white blood cell aggregates was observed shortly
after. his admission. This finding reflects a state of pulmonary leukoaggregates, which
are a pathophysiological component of ARDS.
Early detection of impending deterioration based on the state of leukocyte
adhesiveness/aggregation (LAA) in the peripheral blood can help in the assessment of the
pulmonary status of severely injured patients.
In animal models of severe burn trauma the LAA state (1, 2) has shown a high correlation
between positive peripheral blood findings and lung pathology (3). The test also
correlates well with disease activity (4). Herein is presented the first case report in
which the subsequent development of ARDS was predicted before, clinical, roentgenological
and biochemical evidence existed showing the typical findings of ARDS.
Case Report
A 19-year-old male suffered a 90%
(2nd- and 3rd-degree) BSA burr! injury, with no evidence of smoke inhalation. Fluid
resuscitation was begun. Escharotomy was performed over the areas of 3rd-degree burn, and
silver sulphadiazine cream was used to cover all the burned areas. The patient was
haemodynamicaly stable, in full consciousness and with spontaneous breathing.
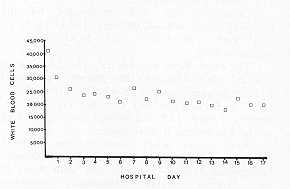
Laboratory data were remarkable for the following values: WBC 42,000/mm, H13 11.9 g/dl;
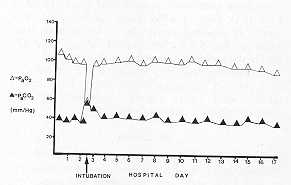
Ph 7.31; Pa02 105; PaC02 36.6; HC03 18.5; 02 saturation 98%.
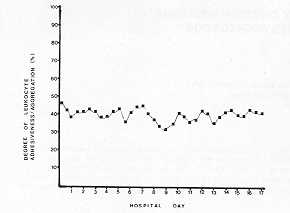
The chest X-ray was normal. The LAA values revealed that 45% of the patient's peripheral
leukocytes were clustered in aggregates (the normal value is from 3 to 5%) (2, 5, 6). The
test was performed every 12 h and showed consistently high levels of peripheral
leukoaggregates.
Sixty hours after. admission the patient's condition deteriorated. He became obtunded,
tachypnoeic (breath 45/min), and with signs of h4emodynamic instability. Laboratory
assessment revealed WBC 22 '000/inin 3 , arterial blood gas analysis was (P02 50%) PH
7.19, Pa02 56, PaC02 59, HC03 23, 02 saturation 81%.
Chest X-ray revealed mild bilateral pulmonary infiltrates. At this time the patient was
intubated and mechanical ventilatory support was given (PEEP of 8 cm H20, Fi02 of 40%).
There was no evidence of sepsis, as repeated blood and tissue cultures were negative. The
LAA state showed values of 4Q-50% during the entire period of hospitalization.
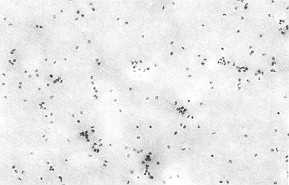
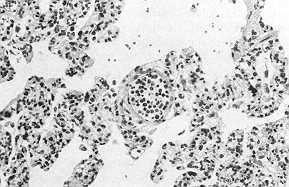
Seventeen days after admission the patient died in a state of cardiopulmonary arrest. Lung
biopsy taken soon after , death revealed multiple leukoaggregates in the lung vasculature.
Discussion
We have observed that a rapid rise in the
LAA percentage to a level ten times higher than normal in most cases indicates the
presence of leukoaggregates obstructing the pulmonary vasculature.
A similar pathology was found in this severely burned patient. As expected, a considerable
elevation of the LAA percentage accurately predicted impending respiratory failure at a
time when the patient was clinically still stable.
The LAA state remained constantly high during the course of the disease and reliably
reflected the patient's status. However, the white blood cell count declined, and the
patient was stable under ventilatory support. The test is simple, sensitive and can be
carried out rapidly (4-7).
The relationship between the presence of pulmonary leukoemboli and ARDS has been well
documented in the literature, and this phenomenon is an important pathological component
in the evolution of the syndrome (8-12). Several studies have shown that ARDS can develop
in neutropenic patients (12-13). This finding is consistent with the generally accepted
theory that leukoaggregates plugging the lung vasculature represent only one aspect of the
pathophysio logical picture of ARDS.
Obviously our procedure will be of limited usefulness in the monitoring of such patients.
The rapid rise in the level of leukoaggregates in the peripheral blood following severe
trauma is due to the development of "stickiness" between white blood cells. This
same process causes the white blood cells to adhere to the endothelium.
The "stickiness" develops as a consequence of the presence of various mediators
in the blood stream during the early post-traumatic period. These mediators (C5a, LT134,
IL-1, TNF-, GM-, CSF) (14-17) are considered to be potent leukoaggregators. On the other
hand the exposure of specific 4migenic components on the surface. of the leukocyte also
serves as a crucial step in the cell-cell interaction (18-22).
RESUME. Les Auteurs
pr6sentent le cas d'un patient avec brillures en 90% de la surface, corporelle qui a
contract6 la syndrome de d6tresse respiratoire aigu6 de I'adulte (SDRA) 60 heures apres la
br6lure~ a la fin it est mort. Peu apres I'hospitalisation its ont observ6 un taux tres
6lev& des agr6gats des leucocytes, cc qui incliquait une condition de
leucoagr&gats pulmonaires qui sont une composante pathophysiologiclue de la SDRA. La
d6tection pr6coce d'une deterioration imminente bas6e sur la condition de
I'adh6sion/agr6gation leucocytaire dans le sang p&riph&rique est utile pour
1'evaluation de 1'6tat pulmonaire des grands br6l6s. C'est le premier cas ou
1'&volution successive en SDRA a 6t& prevue avant que cette possibilit6 ne soit
sugg6r6e par les 6vidences clinique, roentgenologique et biochiniique.
BIBLIOGRAPHY
- Berliner S., Sclarovsky S., Lavie G. et al.: The
leukergy test in rheumatological diseases. New implications for an old test. Arth. Rheum.,
28: 899-903, 1985.
- Berliner S., Fishelson Z_ Bruchis S. et al.: The
phenomenon of leukergy: Induction and detection of leukocyte aggregation in whole human
blood. J. Lab. Clin. Med., 109: 575-582, 1987.
- Fried M., Berliner S_ Ben-Hur N. et al.: Early
detection of inflammation by means of leukocyte adhesiveness/aggregation: a model of burn
in mice. Submitted for publication.
- Berliner S., Fried M., Caspi D. et al.: Evaluation
of disease activity in rheumatic patients by use of the state of leukoeyte
adhesiveness/aggregation. Arm. Rheum. Dis., 47: 458-462, 1988.
- Berliner S_ Caspi D., Neuman Y. et al.: Aggregation
of white cells and C-reactive protein: Relation between these two indices in acute phase
reaction. J. Clin. Pathol., 40: 103-106, 1987.
- Berliner S., Fucks J., Seligsohn U. et al.: Possible
role of fibrinogen in the aggregation of white blood cells. Thrombosis and hemostasis, 58:
749-752, 1987.
- Berliner S., Sclarcivsky S_ Lavie G. et al.: The
leukergy test with ischemic heart diseases. Am. Heart. J., 111: 19-22, 1986.
- Editorial: Neutrophils and adult respiratory
distress syndrome. Lancet, 2: 790-791, 1984.
- Rinaldo J.E.: Mediation of ARDS by leukocytes.
Chest, 89: 590-593, 1986.
- Powe I.E., Short A., Sibbald W.J. et al.: Pulmonary
accumulation of polymorphonuclear leukocyte in the adult respiratory distress syndrome.
Crit. Care. Med., 10: 712-718, 1987.
- Weiland J.E., Davis W.B., Hotter J.F. et al.: Lung
neutrophils in the adult respiratory distress syndrome. Am. Rev. Res. Dis., 133: 218-225~
1986.
- Laufe M.D., Simon R.W., Flint A. et al.: Adult
respiratory distress syndrome in neutropenic patients. Am. J. Med., 80: 1022-1026, 1986.
- Maunder F.J., Hackman R.C., Riff El et al.:
Occurrence of the adult respiratory distress syndrome in neutropenic patients. Am. Rev.
Res. Dis., 133: 313-316, 1986.
- Duchateu M., Haas H., Schreyen L. et al.: Complement
activation in patients at risk of developing the adult respiratory distress syndrome. Am.
Rev. Res. Dis., 130: 1058-1064, 1984.
- Moore F.D., Davis C., Rodrick M. et al.: Neutrophil
, activation in thermal injury, as assessed by increased expression of complement
receptors. N. Eng. J. Med., 3 14: 948-953. 1986.
- Arber N., Aronson M., Berliner S. et al.: Increased
leukocvte adhesiveness/aggregation (LAA) in mice treated with recombinant
granulocyte-macrophage colony stimulating factors (RGM-CSF). Blood, 72: suppl. 1-108a,
1988.
- Pohlman T.H., Stanness K.A., Beatty P.G. et al.: An
endothelial cell surface factor(s) induced in vitro by lipopolysaccharide,
interleukin 1, and tumor necrosis factor increases neutrophil adherence by a CDW
18-dependent mechanism. J. Immunol., 136: 4548-4553, 1986.
- Bevilacqua M.P., Pober J.S., Mendrick D.L. et al.:
Identification of an inducible endothelial-leukocyte adhesion molecule. Proc. Nat. Acad.
Sci. USA., 84: 9238-9242, 1987.
- Schwartz B.R., Harlan J.M.: Neutrophil membrane
sulfhydryl groups are involved in stimulated neutrophils' adherence to endothelium. J. of
Leukocyte Biol., 45: 177-189~ 1989.
- Zimmerman G.A., McIntyre Y.M.: Neutrophil adherence
to human endotheliurn in vitro occurs by CDW 18 (Mol, MAC-I/LFAl/GP 150, 95)
g I ycoprotein -dependent and independent mechanisms. J. Clin. Invest., 81: 531-537, 1988.
- L.,Yarbrough W.C. Jr., Mason C.M., Brite W.M. et
al.: Increased expression of the adhesive glycoprotein CD I I on polymorphonuclear
leukocytes in adult respiratory distress syndrome. Am. Rev. Pes. Dis., 139: A221
(Abstract), 1989.
- Osborn L.: Leukocyte adhesion to endothelium in
inflammation.'Cell, 62: 3-6, 1990.
|