| Annals of the MBC - vol. 4 - n' 2 - June 1991
A STUDY OF BURNS IN CHILDREN
Benito Ruiz J., Navarro Monzonis A.,
Montahana Vizcaino J., Mena Yago A., De La Cruz Ferrer L.I., Mirabet Ippolito V,
Department of Plastic Surgery and Burn
Centre, Hospital La Fe, Valencia, Spain
SUMMARY. A
retrospective study was made of all cases of burns in children admitted to a Burns Centre
over a 4-year period. An analysis is made of the site of injury, mortality, age, sex
ratio, the causes and the place of the accident. Stress is laid on the importance of
prevention campaigns and some guidelines are laid down.
Introduction
Thermal injury is one of the most
frequent accidents in childhood. Although many of these injuries are minor and great
improvements have been achieved in the field of burn care, morbidity (psychic and physical
consequences) from these injuries is important. This means that most of our efforts for
burn prevention should address children ' Since there are differences regarding causes
depending on socioeconomic classes and geography, epidemiological reports are necessary to
establish the target populations for a prevention campaign. Since there had been no such
studies in our area, we carried out a review of burned children admitted to our Centre in
a 4-year period.
Material and results
710 clinical charts of patients
admitted to our hospital were reviewed. 331 (46.6%) were children aged under 15 years old.
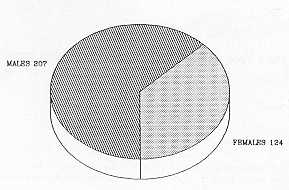
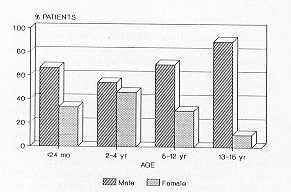
The average age was 4.4 years and the average burn size was 10%. The male/female ratio was
1.5:1. Males outnumbered females in all ages, but the older the patients, the more
numerous the male 220 patients (66%) needed in-hospital care from the very beginning. The
rest were admitted later in the course of their disease. The average length of stay was 10
days. population (Figs. I and 2).
 |
 |
| Fig. 1 |
Fig. 2 |
|
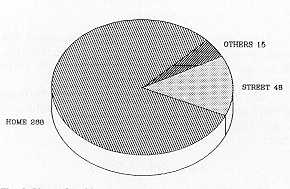
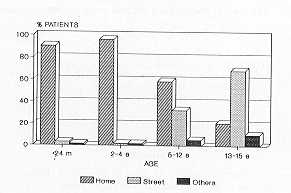
Most of the accidents occurred in an
indoor setting (home) (Fig. 3), but the older the child, the fewer accidents at home and
the more accidents in the street (Fig. 4). The place of accident is related to the cause.
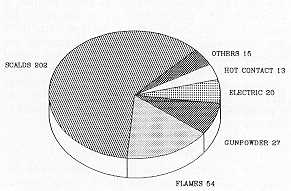
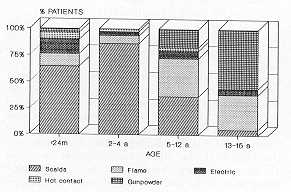
Scalds are the most frequent cause of thermal injury. (6 1 %) (Fig. 5), affecting infants
and toddlers in the kitchen. Flame burns are infrequent in young children but they
increase as they grow older. Gunpowder is the leading cause of injury. in teenagers (Fig.
6).
Scalds accounted for 00% of the thermal
injuries in children under I year old, 8 1 % in children between I and 2 years old, and
84% in children between 3 and 4 years old. The most numerous group injured was constituted
by children between I and 2 years old (90 patients).
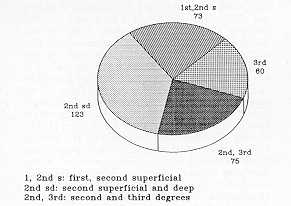
With regard to burn depth (Fig. 7), nearly 40% of the children had sustained
full-.thickness burns to a varying extent.
|
Fig. 7 Bum
depth |
|
Tab. I shows the involvement of th e
different parts of the body. The upper trunk is the commonest site of injury, followed by
the lower limbs. The head, neck and upper trunk form the characteristic pattern of scalds
caused by hot liqu I ds. Burns in the buttocks, genitalia and lower limbs (thighs and
feet) are due to baths. The genitalia are also involved by explosions (due to keeping
firecrackers in trouser pockets).
Mortality
There were 7 deaths. Most of the
deceased had burns covering , 30% TBS (6 patients). Flames, as in adults, were the leading
cause of injury in these patients.
Tab. 2 depicts a comparative analysis between patients under. and over 15 years old. The
difference is not statistically significant, but there is a slightly higher mortality in
adults.
Associated conditions
These are shown in Tab. 3. Corneal
injuries are the commonest and they are related to firework explosions.
Morbidity
Only 30 patients had an accurate
record of microbiological cultures. The isolated specimens are shown in Tab. 4.
Microbiological samples (by swab) were usually taken from patients with full-thicknes
Another 22 patients had to wear this garment as preventive therapy. We cannot provide an
accurate, statistical estimate of success with pressure garments as the results are very
random.
82 patients presented significative sequelae in the form of hypertrophic scars and/or
keloids. 16 of these were scar retractions which provoked a functional limitation. The
rest (66 patients) underwent a programme of physical therapy (pressure garments).
Head and neck
...................................
Face
...................................................
Trunk
..................................................
Upper limb
.........................................
Hands
.................................................
Lower limb
........................................
Genitalia, buttocks
.............................
Tongue
...............................................
Lips
....................................................
Whole body surface
...........................
Anterior body half
.............................. |
116 cases 84
142
116
55
125
41
8
2
5
2 |
Table 1 Site of
injury |
|
BURN
SIZE |
15 yrs, 30% |
15 yrs, 30% |
p* |
| |
TBS |
TBS |
|
| 30 - 50% |
2/21 (9.5%) |
11/53 (20.7%) |
0.2 |
| 51 - 70% |
0 |
6/9 (66.6%) |
- |
| 71 - 90% |
2/3 (66.6%) |
3/8 (37.5%) |
0.4 |
| 91% |
2/2 (100%) |
6/7 (85.7%) |
0.7 |
| TOTAL |
6/26 (23%) |
26/77 (33.7%) |
0.2 |
NOTE:
n/m (%) = n refers,to number of deaths, m to total number of patients in each group, % to
the rate of mortality.
* : significant for p 0.05. TBS: total body surface, |
|
| Table 2 |
|
Epilepsy....................................
Mental retardation.....................
Hydrocephaly............................
Malnourishment........................
Comeal lession.........................
Thoracic trauma........................
Bone
fractures.......................... |
3 patients 2
1
1
7
2
2 |
Table
3 Associated diseases |
|
Catheters:
Escherichia Coli.....................
Staphylococcus aureus...........
S. epidermidis........................
Blood cultures:
S. epidermidis........................
S.
aurcus...............................
Burn surface.:
E. coli
.................................
S. faec.alis ..........................
P. aeruginosa ......................
S. aureus ............................
S. epidermidis.....................
Enterobacter.......................
Acinetobacter.....................
Candida
parapsilosis..........
tropicalis..............
Serratia sp . ........................ |
1
1
3
2
1
5
6
11
16
7
5
4
1
1
1 |
Table
4 Microbiology |
|
Table 5 Preventive guidelines
Do not leave infants or children
unattended. Keep an eye on them, especially in the kitchen. Try to prevent children from
staying in the kitchen if the oven is being used.
Keep kettles, cups, jugs, pans or other utensils with hot liquid or food out of reach and
with 'handles turned towards the wall.
Children tend to imitate everything adults do. Avoid handling or carrying hot liquid or
food in their presence.
Check the temperature of baths, and of food before, serving it. Meals should be lukewarm,
not hot.
Avoid using a tablecloth when there are hot pots on the table. A child could pull it off.
''
Do not have a child on your lap while drinking or preparing a hot beverage (coffee,.tea).
The child could spill it over.
Keep bottles of bleach or other chemical cleaners in safe places and always out of reach.
Put dummy plugs in outlet plugs.
Teach children that fireworks are dangerous and that there are hazards of severe injuries.
Teenagers should be advised to keep firecrackers in a bag or other container and not in
the pockets of trousers or jackets. If fir ' eWorks are not kept on the person they can be
thrown away if they go off accidentally.
Comments
Although we expected otherwise, our
results are surprisingly similar to other reports. 46% of the patients admitted to our
hospital with bum injuries during the 4-year period were children under 14 years old. This
is consistent with the rate given by other authors (1, 2, 3, 4). Male predominance is the
rule and is more significant in older children (5, 6). In our study the ratio male/fem~le
abruptly increases from 2:1 in children under 1 year old to 8:1 in the adolescent group.
Children under 5 years old are at most risk (69% in our series), especially from birth to
2 years old (46%). This is in agreement with other studies (1, 3-9).
Scalding is without any doubt the leading cause of thermal injury. (1, 2, 3, 5, 6, 7, 9,
10, 11, 12). However, as a result of preventive measures, scalding has been overtaken by
other causes in some developed countries(4). Hot liquid continues to be the main cause of
scalds, although there are some geographic differerices (10, 13, 14). For instance, in our
area the main causes of scalds by hot liquid are soups, and water to cook paella or to
prepare coffee.---Boiling oil from saucepans while cooking is another frequent cause. In
Italy accidents with water used to prepare tomato sauce are not uncommon (8), and in
England the main cause is water from kettles for ~he making of tea or coffee,(9).
An important problem regarding bums in children is the risk of t ' he development of
hypertrophic scarring. This was recorded in 25% of our cases. Physical therapy was
prescribed for Most of these children. The results are however very ditTicg.lt to
evaluate. In general terms pressure garments seem to be beneficial, but it is quite
impossible to ascertain if payents and children follow the treatment properly. As pointed
out by Spurr and Shakespeare (15), the therapy is long-lasting, inconvenient and a little
expensive. In addition to this, we live in a Mediterranean area, and hot weather makes
these garments even more uncomfortable to wear.
Finally we-should consider the problem of how to prevent these accidents. First of all.,
it is useless to try to put the blame on anybody. Accidents in infants and toddlers occur
because of the natural curiosity of the child who wants to touch and see everything (to
explore the outer world) and the ignorance of parents and child-minders, who do not think
such accident can ever happen to their children. There are two important points: lack of
proper education and lack of motivation. Parents, child-minders and children have to be
motivated to think that the hazard is possible and that nobody is safe, and they have to
be taught how to avoid these accidents. There are no uniform results regarding preventive
programmes carried out in other countries. Many programmes have failed to reduce the
incidence of bu ' ms (9, 14), whereas others have been succeessful (2, 4). Failure is
probably due to the dlfficq ' Ities of changing habits and lifestyle (12, 13) and the
actual planning of the prevention campaign. Everybody agrees on the target population and
how to educate it through kindergartens, schools, talks, and messages by the mass media
(2, 9, 16, 17), and also by re-education of family doctors and medical students(13). If we
examine failed prevention programmes it seems clear that short-lasting, sporadic and
inconsistent campaigns are condemned to fail.. The only way to achieve good results would
appear to be a long-lasting (maybe permanent), continuous and well-planned campaign.
Linares and Linares (14) recommended the following points to be taken into consideration
when planning a prevention protocol:
- accurate statistical evaluation of regionspecific hazards
- educational programmes which consider motivational factors
- environmental control/product modification through
education and legislation
- a burn prevention office. In each bum unit with competent
and motivated personnel to coordinate local burn prevention effor~s
- responsible authorities who understand the problem and
authorize adequate funds.
We have not yet carried out an effective,
serious programme of p~evention. Tab. 5 shows the main recommendations we give to parents
to prevent thermal injuries. A preventive policy in our community could be drawn up,
including the following points:
- health education in schools, as a compulsory subject,
concerning not only bums but also the prevention of ca ' rdiovascular diseases, cancer,
drug addiction, etc. Of course, the results of such a programme could only be evaluated in
the very long run
- conferences on the prevention of domestic accidents, for
parents, child-minders and teachers
- paediatric and family doctors have a privileged position to
influence mothers and families and try to motivate them. Written information (leaflets
booklets) could be prepared and distributed to families
- health authorities should be persuaded that the economic
expenses of , the prevention programme would be offset.by the reduction of costs for the
treatment of fewer burns.
RÉSUMÉ. Une étude
retrospective a été réalisée de tous les cas de brúlures chez les enfants
hospitalisés dans un Centre de Brúlés pendant une période de 4 ans. Les Auteurs
analysent le site des lésions, la mortalité, Páge, le rapport'garQons/filles, les
causes et le lieu de l'accident. lls soulignent Pímportance des campagnes de prévention
et i1s font, des recommandations utiles.
BIBLIOGRAPHY
- Borrego Galan A., Nuñez Serrano A.: Estudio
elinicoepidemiológico de las quemaduras leves y moderadas en una consulta externa de
cirugía plástica y quemados. Rev. Salud Publ. Castilla y Le6n, 1: 101-106, 1987.
- Landi G., Arcangeli F.: The prevention of bu * rns
in pediatrics:10 years' activity in the Cesena area. Annals of the MBC, 1: 35-37, 1988.
- Haberal M., Onez Z., Bayraktar H., Bilgin N.:
Epidemiology of adults' and children's burns in a Turkish burn center. Burns, 13: 136-140,
1987.
- Lindbald B.E., Terkelsen C.J.: Domestic bums among
children. Bums, 16: 254-256, 1990.
- East M.K., Jones C.A., Feller I., Saxon M.I., Wolfe
R.H.: Epidemiology of burns in children. In: Carvajal H.F. and Parks D.H. (Eds.),
Pediatric bum management. Year Book Medical Publishers, 3-10, Chicago, 1988.
- Rossignol A.M., Locke J.A., Burke J.F.: Paediatric
bum injuries in New England, USA. Bums, 16: 41-44, 1990.
- Barisoni D., Bortolani A., Marchi A.: Epidemiology
and prevention of burns in children. Annals of the MBC, 1: 27-28, 1988.
- Amico M., Caputo G., Geraci V., Ferrara M.M.: 10
years of bums in children: a statistical study with a view to a prevention campaign.
Annals of the MBC, 1: 41-4, 1988.
- Bradshaw C., Hawkins J., Leach M., Robins J.,
Vallance K., Verboorn K.A.: Study of childhood scalds. Bums, 14: 21-24, 1988.
- Klasen H.J., ten Duis H.J.: Changing patterns in the
causes of scalds in young Dutch children. Burns, 12: 563-566, 1986.
- loannovich I., Alexakis D., Panayotou P., Siamaga
E., Papastratis G.: Epidemiological data on burn injuries in Greece: a statistical
evaluation. Annals of the MBC, 1: 23-26, 1988.
- Jamal Y.S., Ardawi M.S.M., Ashy A.R.A., Shaik S.A.:
Paediatric burn injuries in the Jeddah area of Sa , udi Arabia: a study of 19.7 patients.
Bums, 16: 36-40, 1990.
- Keswani M.H.: The prevention of bpm injury, Bums,
12: 533-540, 1986.
- Linares A.Z., Linares H.A.: Bum prevention: the need
for a comprehensive approach. Bums, 16: 281-285, 1990.
- Spurr E.D., Shakespeare P.G.: Incidence of
hypertrophic scarring in bum-injureo children. Burns, 16: 179-181, 1990.
- Brienza E., Di Leonardo A., Minervini C., Portincasa
A.: The prevention of accidental burns at home: a proposal for a new protocol. Annals of
the MBC, 1: 29-33, 1988.
- Silverstein P., Wilson R.: Prevention of pediatric
burn injuries: In: Carvajal H.F. and Parks D.H. (Eds.), Pediatric burn management. Year
Book Medical Publishers, 11-24, Chicago, 1988.
|