| Annals of the MBC - vol. 4 - n' 2 - June 1991
NEUROLOGICAL DISORDERS FOLLOWING ELECTRICAL BURN INJURIES
Lochaitis A., Parker I, Stavropoulou V.,
PanaVotaki D.
Department of Plastic Surgery and Burns,
General Hospital of Attica (K.A.T.), Athens, Greece
SUMMARY. Two
cases are described of the infrequent complication of neurological disorders due to
progressive spinal cord involvement following electrical injury. The possible mechanisms
of this type of damage are discussed.
Introduction
The first recorded case of
electrical injury after the discovery of the electrical phenomenon occurred in 1746 when
two Dutchmen were injured by the accidental discharge of a L,eyden jar. Since then, the
mechanisms by which damage is caused by electric current in the human body have been a
matter of controversy. They are still not fully understood but the unfortunately large
number of electrical accidents both in the home and at work, comprising 3% of all burn
admissions in the USA, makes research in this matter.
At the General District Hospital of Attica a total of 90.5 burn cases were admitted
between 1986 and 1988. Of these, 23 were electrical injuries (2.5%) (Fig. 1). Most
were due to 220 V alternating current in household accidents although some were due to
high-tension current (above 20,000 V) on building sites or in other related jobs.
The effect of current on the nervous system has been well-documented and its sensitivity
to electrical damage is commonly seen. This can take the form of cerebral or spinal cord
lesions or peripheral nerve damage.
Over the past 4 years a variety of neurological pictures have emerged from our unit,
complicating electrical burns. They range from localized single nerve paresis through
multiple peripheral., nerve lesions, localized lesions of the brain such as cerebellar
ataxia after, electrical injury through the skull, more generalized brain damage and
spinal cord lesions which have in some cases been transient but which in two cases, with
delayed onset, left More permanent damage.
In this paper these two cases of progressive spinal cord involvement after electrical
injury are presented, partly because of the infrequency of this complication and partly to
discuss possible mechanisms of such damage.
Case reports
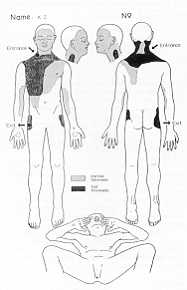
Case I (Fig. 2)
|
Fig. 2
Distribution of burns: case I |
|
On August 4 1988 a 32-year-old policeman
sustained electrical injury while installing a television aerial which accidentally
touched an overhead high tension cable carrying approximately 22,000 V. The patient lost
consciousness but recovered on the way to a general hospital in Athens where he was
admitted and given shock resuscitation. His general condition was good with no signs of
cardiovascular, respiratory or neurological involvement. His burn injury was 25% T13SA and
consisted of full-, and partial-thickness burns as shown. Small charred areas on the right
side of the neck and right hip suggested the entrance and exit points of the current.
On transfer to the Burns Unit of th.e General Distrct Hospital of At.tica, resuscitation
was continued with good response. Escharotomics were carried out on the neck to relieve
the extensive oedema which had formed. Neurological examination was negative and X-rays
showed no sign of skeletal damage.
Three days later the patient noticed weakness of his right hand when trying to hold a pen
or fork but, having occlusive dressing on both arms, did not pay special attention to this
initially. This weakness worsened, however, progressing to the left side and the patient
was no longer able to feed. himself. Maximum deterioration was approximately 15 days
post-burn. Electromyograms of the right arm were negative. During this time weakness of
the legs had also increased and, as in the arm, the first ' find ' ings went unnoticed
until the patient tried to stand. Characteristically, sensation was retained at all times
but reflexes were increased and the Babinski sign was positive.
At 25 days the patient underwent surgery and full-,thickness areas were grafted, After
this there was gradual improvement of his quadriparesis and at 6 weeks post-bum he was
able to walk a few. steps assisted while upper limb function improved more rapidly than
that of the lower limbs.
The patient was discharged after , 8 weeks to continue physiotherapy and neurological
follow-up as an out-patient. Improvement has been gradual over the year and although the
patient walks well and upper limb function is very good, neurological examination still
reveals evidence of spinal cord lesion at the level of C4-C5 involving selective pyramidal
tracts with increased reflexes, some clonus and slight spasticity.
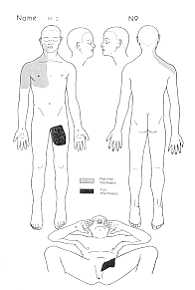
Case 2 (Fig. 3)
|
Fig. 4 Types
of electrical injury.
Electrothermal bum - due to arc
- Flame bum - due to ignition of clothes, etc.
- Deep thermal bum - due to current conduction along
pathway of least resistance in body
- "Crush" injury. - due to cellular and
ischaemic damage from the current
|
Fig. 3 Distribution
of burns: case 2 |
|
A 43-year-old Yugoslav working for ' the
Greek electrical company in the north accidentally came into contact with high tension
cables causing him to be thrown from a height of 4 M.
On admission to the nearest hospital, the patient was conscious and found to have 10%
burns, chiefly partial-thickness, of the face, right upper arm and a small area of the
left thigh, without any of th ' ese indicating the exact entrance and exit points of the
current. He also had a fractured left femur and 8th right ' rib. ECG revealed a right
bundle block which quickly righted itself. Neurological examination revealed paresis of
the right radial nerve. He was transferred immediately to the Bums Unit of our hospital
where the clinical picture was the same.
The follgwing day the patient complained of weakness of both lower limbs which progressed
rapidly upwards showing almost complete paraparesis within the next 2 days.
Characteristically sensation was fully retained as well as proprioception. Reflexps were
again increased and signs for pyramidal damage were positive. Since there was initially
some doubt as to whether the neurological picture might in fact.be due to damage to the
vertebral column, the patient was then transferred to the Orthopaedic Unit for full,
investigations.
Laboratory and radiological investigations were all negative, as was the myelogram and CT
scan of the spinal cord, and though his paraparesis remained essentially unchanged the
patient began to show increased tendon reflexes in both upper limbs, indicating the
continuing progression of hi.S spinal cord lesion.
Immediately after, completion of in ' vestigations the patient was transferred at his
request to Yugoslavia, thus making follpw-up of his case impossible.
Discussion
The effects of electric current on
the human body have been generally well-documented, though numerous factors are involved
which will affect , the type and extent of the damage caused. It is well known that there
are basically fou~ types of electrical injury. (Fig. 4):
- The electrothermal burn,
caused by arcing of the
current from the source to the body and usually affecting the skin only in varying depth
and extent. This is usually foupd where high-voltage current is involved.
- The flame burn,
usually caused by ignition of the
clothes, again of varying extent and depth.
- The deep thermal burn,
due to conduction of the current
along the pathway of le , ast resistance, causing tissue destruction often.far more
serious than surface. burns suggest.
- The "crush" type of injury,
which can affect.
any organ of the body and has been attributed to cellular and ischaernic damage from the
current.
With regard to the actual current causing
the accident, again there are many factors which will affect.the degree of injury. (Fig.
5):
Fig. 5 Factors
affect , ing injury. due to the passage of electric current through the
body
- Type of circuit and current
- Voltage of circuit
- Resistance of tissues
- Amperage of current
- Pathway of current through the body
- Duration of contact
|
|
1) Type of circuit and current
Experimental studies have shown (Lee
and Kolodney, 1987) the importance of the type of ci~Cuit created when current flows
through the body. When a voltage is applied across the body the rate of heating of each
tissue through which current passes depends not only on the properties of the tissue
themselves but also on their arrangement within the circuit.
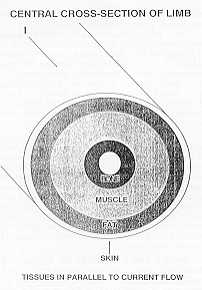
If th , e tissues are in series the
current density is identical but the fielq strength is differqpt in each tissue and
heating is inversely proportional to tissue conductivity. In parallel, as we see in the
cross-section of the limb (Fig.6), urrent density varies with each type of tissue, with
the layer having the highest conductivity experiencing the highest temperature rise. We
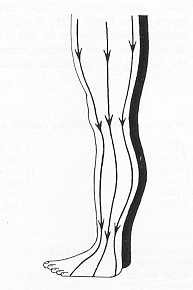
can also see (Fig. 7) that current density in differptit areas varies, being most
concentrated near the joints and inversely proportional to the cross-sectional area of the
limb. Thus the quantity of heating produced in electrical injury. is dependent on tissue
conductivity, current density and the relationship of tissues to the current flowing
through them.
It should also be remembered that the type of current, alternating or direct, will also
affect the injury, low-voltage AC usually causing more damage than the equivalent DC,
though high-voltage DC is more frequently fatal.
2) Voltage
Potentials of les , s than 24 V are
usually considered safe. High-voltage accidents usually cause devastating injuries. It is
interesting to note that all recorded instances of spinal cord damage are from
high-voltage circuits.
3) Resistance (Fig. 8)
It is quite well known that tissues
offer.yarying resistances to electric current and it has always been i thought that
heating is greater in tissues of high resistance (Baxter et al.). However, Lee and
Kolodney in an experimental model of the upper limb where tissues are in parallel fou4d
that the greatest temperature rise when 4 V was applied was in tissue of lowest
resistance.
 |
 |
| Fig. 6 |
Fig. 7 Current
density is concentrated at joints |
 |
Fig. 8 |
|
4) Amperage
This is of extreme importance.
Currents of greater than 15 milliamperes are sufficiqnt to cause nerve and muscle
stimulation and tetanic contraction and currents of over 60 milliamperes usually cause
ventricular fibrillation.
5) Pathway (Fig. 9)
It is generally observed that where the
current passes from hand to hand the mortality rate is high, about 60%, whereas in the
head to foot. pathway it is only about 20%. There is an increase of spinal cord injury.
usually between the levels of C4-C5 when the current passes from hand to hand.
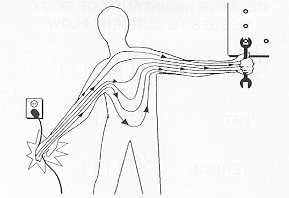 |
Fig.
9 Current lines through body if current passes arm-to-arm |
|
6) Duration of contact
The longer the duration of contact the
greater the damage.
Spinal cord involvement (Fig. 10) is one of the less common neurological complications and
statistics vary as to the frequency of its appearance. Panze (1930), Hyslop (1949),
Silversides (1964) and Jackson (1964) all described such cases. Varghese et al. (1986)
described 5 cases of spinal cord injury, out of I 16 patients with electrical injury.
(4.3%). Others place this incidence much lower, though possibly some milder cases go
unrecognized or are attributed to limb weakness from generalized immobilization and
prolonged bed rest. The two cases presented here amongst 23 electrical bums admitted
during the past three years represent a percentage of 8.~%.
Appearance of neurological disorders of this type can be immediate but usually varies from
a few,days to a few weeks after.injury, although it has been noted up to two years
afterwards (Levine et al., 1975; Farrell et al., 1986). Prognosis would seem to be related
to the delay of o.nset, being worse when this is considerable, varying from complete
recovery to, very rarely, death. Jackson et al. (1964), Holbrook et al. (1970),
Christensen et al. (1980) and Varghese et al. (1986) have described 40 cases of delayed
onset spinal cord involvement where partial recovery was seen in only two patients, while
in 27 cases, where the onset was immediate, complete recovery was 100%.
In both our cases there was a small delay in onset, which was after.three days in
the'first. case and after 24 hours in the second. Reasonably good recovery is present in
Case I which is still progressing a year later. Unfortunately Case 2 transferred from
hospital to his home country before. the outcome of his progressive neurological lesion
was known.
Most authors describe these spinal lesions as predominantly motor, taking varying forms.
Panze in 1931 described it as "spinal atrophic paralysis" and it can take a form
consistent with ascending paralysis, transverse myelitis or amyotrophic lateral sclerosis.
Taking into consideration the factors affecting injury. when electric current passes
through the body, as already described, the necessity of find , ing an explanation for the
cause of injury. now arises. This can be summarized as follows (Fig. 11):
Trauma. The possibility of direct trauma to the spinal cord, caused either by the
patient being thrown by the current or by violent tetanic muscle spasms, cannot be ruled
out even where there are no radiological find , ings. However, in this case, one would
expect the onset to be immediate, while in our cases it was not. But if we. consider that
the artery walls also contain muscle there is a possibility (Petty, 1986) that tetanic
contraction of this muscle tissue in small arteries supplying the spinal cord and its
roots could cause a delayed atrophy to the nervous system due to impaired blood supply.
Heating. This is caused by the dissipation of electricity in nerve tissue, which
would seem to be a proliferative angiopathy in the vessels surrounding the spinal cord. A
recent theory of Robson et al. is that heating causes injury, to the cell which responds
by producing inflammatory mediators, chiefly Jn the form of thrOmboxane A2, which cause
deterioration, ischaernia and cell death.
Irradiation type injury. This explanation attributes injury, to the direct effect ,
of thp current on the cord which causes changes in the DNA and enzyme systems of nerve
cells affecting mitosis which results in the formation of abnormal proteins in the
endothelial cells of th , e vessels. These changes are similar to those seen after
irradiation. The abnormal cells proliferate within the vessels causing interference with
blood flow.
Fig. 11 Mechanisms
of injury. to spinal cord
- Direct trauma
- Thermal damage
- Vascular damage
- "Irradiation type" changes of DNA and enzyme
systems
- Electrogenic breakdown of cells
|
|
Electrogenic breakdown of cells. In
this complication where neuropathy often , has a delay in onset either of as in our cases,
or even years, other mechanisms of damage must be considered. For instance, myoglobulin
from muscle rupture is usually released after.electrical injury, and histology shows the
adjacent coexistence of normal and damaged cells, a phenomenon difficult to explain by
thermal mechanisms alone. There is evidence too, from some reports such as that of Lee et
al. (1982), that local electrical fiel0s can be sufficipnt to cause breakdown of cell
membranes and thus lysis of the cells with all the pathophysiological consequences. They
also suggest that long cells, such as nerve cells, are perhaps more vulnerable and that
they are most susceptible when arranged in parallel to the passing current. Small perfora
, tions in cell membranes caused by the field are suffici.e.nt to upset the delicate
balance between intra- and extracellular environment and will eventually lead to
destruction of the cell. Both the increased myoglobulin levels and the derivatives of
membrane phospholipids after.electrical injury. Would tend to substantiate this theory of
cell rupture after electrical trauma.
Conclusion
The presentation of su , ch cases is not
new but a study of the literature reveals that cases of spinal cord damage following
electrical injury, are uncommon. Infact, it is a complication which sometimes tends to be
overlooked, especially when the localized thermal damage is either so insignificapt that
it would not be expected or so serious that all efforts are concentrated in that
direction. In our first, case, although upper limb weakness was soon evident, lower limb
deficit , was not really seen until the patient tried to ambulate. In the second case the
neurological problem was quickly obvious since paraparesis developed quickly.
On reviewing the physics involved in the application of an , electric current to the body
and also the possible pathophysiological mechanisms which can explain such injury, it is
obvious that research in this fielO is far from complete. The variations in onset times
for this complication are not entirely explicable nor the selective areas which are
usually affectpd. The retention of sensation seems to be a fairly common characteristic
present in both of our cases, showing selective preservation of the relative tracts.
Since the exact cause of the damage still remains in doubt, so does the treatment or
possible prevention of the development of this often. very serious complication.
RESUME. Deux cas sont
présentés de la complication peu fréqpente de troubles neurologiques dus a la
déterioration progressive de la moelle épiniére aprés une brillure électrique. Les
mécanismes qui peuvent causer ce type de dommage sont discutés.
BIBLIOGRAPHY
- Baxter C.R.: Present concepts in the management of
rn~ajor electrical injury, Surg. Clinics of North America, 50: 1401-1418, 1970
- Christensen J.A., Sherman R.T., Balis G.A., Wuamett
J.D.: Delayed neurologic injury. secondary to high-voltage current, with recovery. J. of
Trauma, 20, 12: 166-168.
- Critchley M.: Neurological effect,§ of lightning
and electricity.Lancet: 68-72, 1934.
- Duis H.J., Klasen H.J., Reenalda P.E.:
Keraunoparalysis, a "specific". lightning injury, Bums, 12: 54-57, 1985.
- Farrell D.F., Starr A.: Delayed neurological
sequelac of electrical injuries. Neurology, 18: 601-606, 1968.
- Holbrook L.A. et al.: Delayed myelopathy: a rare
complication of seyCre electrical bums. Br. Med. J., 4: 659-666, 1970.
- Jackson F.E., Martin R., David R.: Delayed
quadriplegia following electrical bum. Military Medicine: 601-605, 1965.
- Kanitkar S., Roberts A.H.N.: Paraplegia in an
electrical bum::i a case report. Burns, 14: 49-50, 1988.
- LangwWhy O.R.: Neurological abnormalities produced
by: electricity. Journal of Nervous and Mental Disease, 84: 13-26, 1929.
- Lee R.C., Kolodney M.: Electrical injury.
mechanisms: dynamics of thermal response. Plast. and Recon. Surg., 80, 5, Nov. 1987.
- Lee R.C., Kolodney M.: Electrical injury.
mechanisms: electrical breakdown of cell membranes. Plast. and Recon. Surg., 80, 5, Nov.
1987.
- Levine N.S., Atkins A., McKeel D.W. Jr. et al.:
Spinal cord injury. following electrical accidents: case reports. J. Trauma, 15: 459-463,
1975.
- Petty P.G., Parking G.: Electrical injury. to the
central nervous system. Neurosurgery, 19, 2, 1986.
- Robson M.C., Murphy R.C.: A new explanation for
progressive tissue loss in electrical injuries. Plast. and Recon. Surg., 7 5: 43 1, 1984.
- Silversides J.: The neurological sequelae of
electrical injury, Canad. Med. Assoc. J., 91: 195-204, 1964.
- Varghese G., Mani M.M., Redford. J.B.: Spinal cord
injuries following electrical accidents. Paraplegia, 24: 156-166, 1986.
|