| Annals of the MBC - vol. 4 - n' 3 - September 1991
PLASTIC SURGERY RE-EDUCATION IN SEVERELY
BURNED PATIENTS: FROM SURVIVAL TO QUALITY OF LIFE
Caleffl E., Bocchi A., Toschi S., Papadia
F.
Cattedra di Chirurgia Plastica
dell'Universita di Parma, Italia
SUMMARY. In major burns,
surgical procedures have a rehabilitative perspective in each therapeutic step: first,
early debridenient and coverage of the burned areas are necessary for a quicker recovery
and to reduce complications; improper early management ol'burned areas is still the main
cause of scar contractures and disability. Subsequently, an appropriate surgical approach
is often necessary to improve the functional outcome and social reintegration. In a
complete therapeutic approach to the burned patient, each surgical operation must be
associated with conservative treatment, i.e. nutritional, immunological support in the
early phases, and physiatric devices in the post-acute phases. In this way surgical steps
can be reduced and complete rehabilitation be more effective.
Introduction
Plastic surgery re-education in the
severely burned patient includes different surgical steps aimed at ensuring the patient's
survival and permitting further surgical approaches for a better quality of life. We
divide surgical re-education into three phases: 1. Early surgical re-education: this
takes place when the patient is admitted to a Burn Centre and aims at his life support. It
begins with escharectomy to prepare the burned surfaces for skin autografts. These, both
direct autograft and autograft of previously cultured skin, have a quoad vitam purpose
(to repair the skin covering) and also a quoad veletudinem purpose (to facilitate
non-surgical re-education, avoiding subsequent incorrect postures), even though they
sometimes give unsatisfactory aesthetic and functional results. Cultured skin autograft is
an important new re-educative life support, especially in very severely burned patients,
because it allows quite early intervention without creating donor sites. Allografts,
heterografts, and amniotic and collagen membranes, used as biological dressing, have a
minor re-educative meaning as life support because of their temporariness and the high
risk of phlogosis and infection.
Elective surgical re-education: this
concerns grafted or secondary closure healed areas. The re-educative purpose is to obtain
the best individual and social integration of severely burned patients, the ideal result
being to restore, as far as possible, the pre-existing local, functional and aesthetic
conditions. We use:
a) Plastic for elongation and debridement
of scars (Z-plasty, V-Y plasty,, W-plasty) and local flaps, to transfer the same kind of
skin existing before the trauma to the burned area with minirriurn discomfort for the
patient.
b) Expanded skin flaps, to repair
extensive burned areas: two interventions and an expansion tinic are required, but they
allow reintegration of damaged tissues whose reconstruct ion was impossible, or at least
very difficult, in the past~ Cross-abdominal flaps: these still have an important
re-educative role even though the long time required before pedicle separation proves to
be very psychological patients, patients usually are.
Microsurgical flaps: these may give
sensitivity, but have few strict indications and often post-operative complications. In
phase 2 non-surgical re-education is mainly based on dynamic splints, to restore
reconstruct& tissne function.
3. Sequelae surgical re-education.. this
concei-ns surgically treated burned areas and donor sites, developing through
"complementary" or "p rfective" surgical techniques, such as
dertnoabrasion, peeling and punching, which represent a further surgical step.
Another important concept is re-educativc
priority: since severely burned patients have extensively damaged tissue, a carefully
selected re-educative programme is needed: surfaces covcring meta-epiphyscal zones in
children, to prevent growth defects; in adults priority is given to body surfaces useful
to working, then to the treatment of arthral surfaces and finally exposed areas, for
aesthetic reasons,
Clinical data
In the last 10 years 938 burned
patients have been admitted to our Burn Centre: in severely burned patients (50%) with
over 15% BSA the complete three-phase treatment was applied in 215 cases.
We report five cases to illustrate our protocol and to show our results.
Case report I
25-year-old woman with 2nd- and
3rd-degree burns, caused by hot water, in 40% BSA, 25% of which were classified as deep
(sternal and mammary region, upper limbs); early escharectomy and tangential excision wefe
performed and the wounds were covered with skin autografts.
4 years later pre-sternal hypertrophic scars were treated with Z-plasty. 8 years later 2
skin expanders (455 cc each) were introduced into the mammary region. After expansion and
complete scar excision, the expanded skin flaps were used for coverage.
Case report 2
42-year-old male with 3rd-degree flame
bums (extremities, face, neck, chest, upper and lower extremities) caused while attempting
suicide, affecting 50% BSA.
In the early phase meshed and cultured skin grafts were used to accomplish a quick and
complete coverage. 1 year later a tissue expansion was performed in the cervical region to
correct a severe neck contracture.
A Z-plasty of the commissure was carried out 6 months later to enable the patient to play
the trumpet again.
Case report 3
33-year-old woman with considerable
burns of face, arms and hand which occurred at the age of 6 months.
Facial burned areas were repaired with splitthickness skin grafts. 14 years later the
patient was admitted to our hospital for the first time: a tissue expander was introduced
into the right cervical region. The expander skin flap was used to correct the severe
contracture of the lower lip. 1 year later a left cervical expander (730 cc) was
introduced to correct remaining scars of the cheek.
A few months later a chin augmentation was carried out, using osteocairtilaginous tissue
obtained from septorhinoplasty.
A bilateral upper lip flap was also performed to recontruct the commissura labialis.
Finally, reconstruction of the auricular lobe was performed.
 |
 |
| Fig.
la Extensive scars of sternal and mammary region treated with two tissue
expanders |
Fig. lb Post-operative
view after complete removal of sternal and mammary scars and correction with a Z-plasty of
an axillary scar. A correction of ptosis has also been obtained |
|
Case report 4
17-year-old woman with 3rd-degree
burns of chest, BSA. Early escharectomy was carried out and coverage was perforned with
skin autografts. After sexual development, debridement of thoracic scars and remodelling
of left breast with a silicon prothesis were performed. One year later, reduction
mammoplasty on the opposite side was performed. lower extremities and left arm, affecting
40%
 |
 |
| Fig.
2a Severe scar contracture of the neck: pre-operative view |
Fig.
2b Expansion of cervical region previously treated with mesh grafts |
 |
 |
| Fig.
2c Intra-operative view: large expanded flaps were raised and placed in Z-plasty
manner to increase neck surface |
Fig.
2d Side post-operative view with elongation of neck skin |
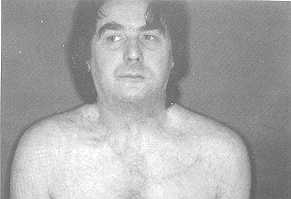 |
Fig.
2e Front post-operative view: a Z-plasty of the commissure has also been
performed |
|
Case report 5
27-year-old woman with 2nd- and
3rd-degree burns of upper extremities and back.
During the post-acute phase in the hand and wrist the patient developed hypertrophic scars
with severe contracture. Finger contracture was corrected with a cross-arm flap (results
shown in our previous work). A few months later wrist contracture was corrected with an
abdominal flap.
Discussion
This different reconstructive techniques in three
subsequent phases, shows the importance of a surgical re-educative approach to obtain
biological and social reintegration for these severely afflicted patients.
 |
 |
Fig. 3a Post-burn scar of the face (chin scars
have already been removed by means of tissue expansion) |
Fig. 3b Final
photograph after complete removal of scar of the face, reconstruction of the auricular
lobe and chin augmentation by osteocartilaginous tissue from septoplasty |
|
In the 'Tarly Surgical Re-education" phase we use
traditional or cultured skin autograft. We have been using the latter since 1989. For
burns between 50 and 70% we employ the two kinds of graft together, whereas cultured skin
is used alone for bums over 70%. The results are very similar, even though the structural
fragility and sensitivity to infection of the cultured skin autograft may affect its take,
causing some delay to the whole re-educative process.
 |
 |
| Fig.
4a Post-burn breast contracture: pre-operative view |
Fig. 4b Post-operative
view after debridement and remodelling of the right breast and reduction mastoplasty of
the left breast |
 |
 |
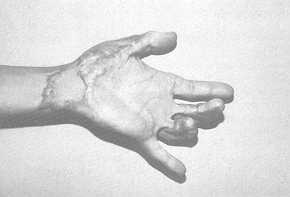
| Fig.
5a Severe contracture of 3rd and 4th fingers and of the wrist. Pre-operative view |
Fig. 5b Post-operative
view after removal of scar tissue of the finger by cross-arm flap and of the wrist by
abdominal flap |
|
If possible, we therefore prefer to
reintegrate functional areas by traditional grafts; nevertheless, cultured skin graft has
the advantage of requiring no donor sites.
In the "Elective Surgical Re-education" phase the extent of the damaged area is
of primary importance: for small areas we prefer basic techniques, like Z-plasties or
local flaps: for larger but circumscribed surfaces we use expanded skin flaps, taking into
account the expandability of the area and the risk of complications (infection, decubitus
of the prothesis).
Of the two distant flaps, cross-abdominal flaps have a lower incidence of post-operative
complications than microsurgical flaps, the failure of which may disappoint the patient,
inducing him to abandon further re-educative programmes. We therefore use microsurgical
flaps only after strict selection on the basis of age, site of burn, and circulatory
integrity.
The Sequelae Surgical Re-education", while exploiting so-called
"complementary" techniques, is of great importance inasmuch as it shows the
interest of burned patients in improvement of their aspect, also as regards aesthetic
considerations.
This represents the evolution from a biological to a psychological healing, which should
be the ultimate purpose of re-educative therapy.
RESUME Dans les brfilures
graves les proc6dures chirurgicales, A chaque pas th~rapeutique, ont une perspective
r66ducative: avant tout, le c16bridement et le recouvrement des surfaces brGI6es sont
nkessaires pour permettre une gu~rison plus rapide et pour r6duire les complications; le
traitement pr~coce impropre des surfaces brdl~es reste toujours la cause principale des
contractures cicatricielles et de I'mvalidit6. Tr6 souvent it est n~cessaire Wintervenir
chirurgicalement par la suite pour anifflorer le r6sultat et la r6int6gration sociale.
Pour aborder en mani~re compl&e la th~rapie du patient brfil~, it faut que chaque
manoeuvre chirurgicale soit associ& A un traitement conservatif, e'est-A-dire it faut
fournir un soutien alimentaire et des supports physioth~rapeutiques dans les phases
post-aiguds. De cette mani~re it est possible de r6duire les proc~d~s chirurgicaux et la
r~adaptation compl&e est plus efficace.
BIBLIOGRAPHY
- Barisoni D.: Le ustioni e it loro trattamento.
Piccin Editore, 1984.
- Baux S.: Traitement des r&ractions des plis de
flexion des membres. Annals of the MBC, 2: 205-207, 1989.
- Baux S.: La place de Pexpansion cutan~e clans les
s6quelles de brfilures. Annals of the MBC, 3: 5-7, 1990.
- Bunkis J., Ryv RK, Walton R.L., Epstein L.l.,
Vasconez L.O.: Fasciocutaneous flap coverage for periolecranon defect. Arm.Plast. Surg.,
14: 361, 1985.
- Calefili E, Bocchi A., Toschi S., Ghillani M.:
Surgical treatment of post-burn contracture of the hand. Annals of the MBC, 3: 12-15,
1990.
- Calefti E, Bocchi A., Toschi S., Montacchini G.,
Papadia E: Tissue expansion in the treatment of burn scars. Third Meeting of MBC, Cairo,
1989 (Abst).
- Casa B., Costa P., Ferraro F., Delpiano P.,
Gasparini G.: Le ortesi nella riabilitazione de¡ paziente ustionato. Gior. Mal. Med.
Riab., 1 (1V): 22-27, 1990.
- Damour 0., Dantzer R., Poinsignon F., Vescovali C.,
Marichy J., Colombel C., Echinard C.: Contróles physicocliniques et experimentaux d'un
derme artificiel á base de collagéne. MBC, 1: 196-199, 1988.
- Davies D.M., Yacournattis A.M.: A method of grafting
hand, burns following early excision. Br. J. Surg., 65: 539, 1978.
- Diamond M., Barwick W.: Treatment of axillary burn
scar contracture using an arterialized scapular island flap. Plast. Reconstr. Surg., 72:
383, 1983.
- Echinard C., Dantzer E, Poinsignon E, Damour 0.,
Vescovali C., David M.F., Marchetti B., Collombel C.: Etude biologique et physique d'un
derme artificiel - biocompatibilit~ chez Panimal. Annals of the MBC, 1: 200-202, 1988.
- Fischer J.: External oblique fasciocutaneous flap
for elbow coverage. Plast. Reconstr. Surg., 75 51, 1985.
- Haberal M., Oner E., Gulay H., Bayzantar U., Bilgin
N.: Severe electrical injury and rehabilitation. Annals of the~ MBC, 1: 121-123, 1988.
- Hallock G.G.: Island forearm flap for coverage of
the antecubital fossa. Br. J. Plast. Surg., 39: 533, 1986.
- Hicagi M., Mandour S., Shalby H.A.: Post-burn
contracture of the axilla. Evaluation of three methods of management. Annals of the MBC,
3: 21-25, 1990.
- Hirshowitz B., Karev A., Rousso M.: Combined double
Z-plasty and Y-V advancement procedure for repair of thumb web contracture. Hand, 7: 29,
1975.
- Lorenzini M., Cristofoli C., Governa M., Rigotti G.,
Barisoni D.: Microsurgical treatment in acute bums and their sequelae. Annals of the MBC,
3: 100-103, 1990.
- Malher D., Benmeir P., Ben-Yakar J., Hauben D.,
Greber B.,Sagi A.: Is early surgical treatment still the best solution for deep burns?
Annals of the MBC, 1: 116-117, 1988.
- Masellis M., Ferrara M.M., Fortezza G.S., Lorusso
P.: Frozen amniotic membrane: a biological covering for superficial burns. Annals of the
MBC, 1: 186-195, 1988.
- Masellis M., Vitale R., Lorusso P. L'amnios
congelato come sostituto bilogico della cute nel trattamento delle ustioni superficiali.
XXXII Congr. Naz.
- S.I.R.C., Tomo If: 1339-1349, 1986.
- Miller T.A., White W.L.: Healing of second degree
bums. Plast. Reconstr. Surg., 49: 522, 1972.
- Sucameli M Geraci V: Ohmori S.: Correction of burn
deformities using free flap transfer. J. Trauma, 22: 104, 1982.
- Osman O.F., Houtah A.M.: Forearm fasciocutaneous
flaps for coverage of defects around the elbow. Annals of the MBC, 3: 84-86, 1990.
- Pousa Rebal F.: Cryopreserved allograft skin to
cover 50% deep burns. Annals of the MBC, 3: 26-28, 1990.
- Roug6 D., Escourrou G., Laguerre J., Conil J.M.,
Micheau Ph., Laffitte F., Chavoin J.P., Costagliola M.: Pour une r6paration pr6coce des
brillures 6lectriques: nt6r6t du concept de 16sions tissulaires extensives. Annals of the
MBC, 3: 90-93, 1990.
- Walton R.L., Bunckis J.: The posterior calf
fasciocutaneous free flap. Plast. Reconstr. Surg., 74: 76, 1984.
- Zdravic F.C.: Priorities and pitfalls in treatment
of bums. Annals of the MBC, 1: 113-115, 1988.
|