| Annals of the MBC - vol. 4 - n' 4 - December 1991
OUR EXPERIENCE WITH A HYROCOLLOID DRESSING (COMFEEL) IN THE
MANAGEMENT OF DONOR SITES
De La Cruz-Ferrer L.I., Mena-Yago A., Benito-Ruiz J.,
Baena-Montilla P., Navarro-Monzonis A., Chamorro-Hernandez J.J.
Department of Plastic Surgery and Burn Centre, Hospital La
Fe, Valencia, Spain
SUMMARY. A trial was made of the
new dressing Comfee~' on 100 skin donor sites. The following parameters were evaluated:
epithelialization time, pain, case of use, and complications. Comfeel was found to be very
satisfactory as it reduced epithelialization time, was comfortable for the patient, and
required few dressing changes. The slight extra expense was outweighed by the advantages.
Introduction
The numerous papers published about
synthetic dressing for the management of donor sites and the good results reported led us
to start a prospective study on this issue in 1988. The traditional dressing in our Centre
for donor sites was tulle-gras plus nitrofurazone.
The trial consisted of using the new dressing (Comfeel-11, Coloplast, Espegaerde, Denmark)
on 100 donor sites, evaluating the following parameters: length of time for complete
epithelialization, pain or itching, case in surgical management and dressing change, and
complications.
Material and methods
The utilized dressing (Comfeel) has a
bilaminate structure. The inner layer is composed of sodium carboxymethylcellu lose, which
is absorbent, and the outer impervious layer is made of polyurethane. We tested the two
kinds of dressings: opaque and transparent.
100 donor sites (86 thighs, 9 arms, 3 buttocks and 2 abdomens) corresponding to 87
patients were studied. The age range was from 14 to 65 years. Patients with any general
disease were excluded. A personal authorization was collected from all patients, data
regarding the above parameters were recorded, and pictures of the entire procedure and
evolution were taken.
Grafts were harvested with a Humby dermatome by the same surgeons (first two authors) to
avoid differences concerning depth of the donor sites which might influence the study.
Immediately after harvesting of the graft, the donor bed was compressed for five minutes
with a lap soaked in 1:300000 adrelanine solution. Good haemostasis is compulsory in order
to avoid postoperative complications. The dressing was then applied, taking the precaution
that It must be larger than the defect in order to allow good adherence of the dressing to
the surrounding, non-injured skin (Fig. 1) (Queen et al., 1987). In 25 patients the
transparent Comfeel was applied (Fig. 2). To enhance haemostasis and provide good
inmobilization, an elastic bandage was applied. The following day the dressing was
inspected to cheek for the presence of haematoma. In this case, a new dressing was applied
on the donor site after clot removal. The first dressing change was done on day 6 after
the operation. The degree of epithelialization was evaluated and the average value was
taken.
If the donor site was not covered completely with new epithelium, a new hydrocolloid
dressing was put on. The second dressing change was between the 8` and 1011 days.
Patients were asked on a daily basis about pain, which was evaluated by a score from 0 to
100. 0 is total absence of pain, and 100 is considered the worst pain ever suffered.
Evaluation of comfort and ease of management of the donor site was accomplished by
interviewing five surgeons and ten nurses.
Results
Time for re-epithelialization of the donor sites
The average time recorded fo r complete
re-epithelialization was 8.2 days. By the first dressing change (6,11 day) 34% of the
donor sites presented an epithelialized surface greater than 90% (Fig. 1). 6 1 % of the
donor sites were nearly healed (>95% of the donor site surface) by the second dressing
change. 5% of the donor sites needed more than two dressing changes to achieve complete
healing.
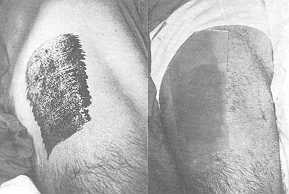 |
Fig. 1.
a) Fresh donor site on right thigh covered with
b) opaque Comfeel. |
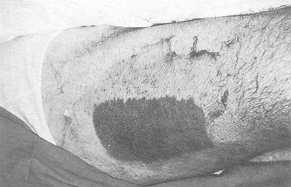 |
Fig. 1. c) Donor
site at the first cheek-off |
 |
Fig. 1. d) Aspect
at six months. |
|
Pain
On average, patients with this new dressing had a pain
score of 18 points. No patient judged the change to be very painful.
 |
Fig. 2. a) Transparent
dressing on a fresh donor site |
 |
Fig. 2 b) Dressing
at day 6. There is no fluid build-up and careful follow-up is possible |
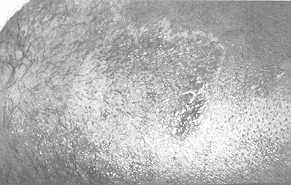 |
Fig. 2. c) The
same donor site at 3 months. |
|
Comfort regarding application (dressing changes)
The surgeons did not find any difference compared to
other dressings with regard to the case of application on the fresh donor site.
80% of the nurses considered the new dressing more comfortable, due to two main reasons.
First, the patient complained less about pain, and second, dressing removal was easier to
perform. Tulle adheres to both wound and surrounding skin, whereas the hydrocollold
dressing attaches only to healthy skin.
Complications
Five donor sites required revision within
the first 24 hours due to haematomas (Fig. 3). These were removed and a new dressing was
put on, without further complication.
An excess of fluid beneath the dressing, causing its detachment, was recorded in seven
cases. The accumulation of fluid happened in these cases between day 2 and day 6.
Only two cases presented clinical infection which required discontinuation of the use of
the dressing and caused delayed healing.
Discussion
The main feature of a dressing should
be its capacity to provide an environment which enhances growth of epithelium on the wound
from the dermal adnexa. Semi-occlusive dressings seem to fulfil this requisite, creating a
moist microclimate with a lower 0, concentration on the surface of the wound. A good
oxygenation at the capillary bed and a fair level of oxygen on the surface are keys to
improve epithelialization (Winter, 1972; Pollack, 1979; Davies, 1984; Hermans and Hermans,
1986; Horikoshi, Balin and Carter, 1986), reducing inflammation (Linsky, Roove and Dow,
1981) and increasing the synthesis of collaaen (Alvarez. Mertz and Ea0estem, 1983).
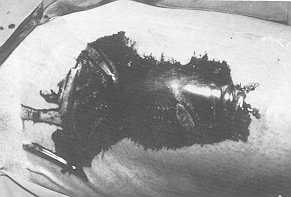 |
Fig. 4. Disepithelialization
occurs as the tulle dressing is removed. The donor area which was covered with the
hydrocolloid dressing is healed. |
 |
Fig. 3. Haematoma
at 24 hours. Transparent dressing allows an early diagnosis. The dressing was removed, the
clot cleaned and a new dressing applied. The donor site healed uneventfully. |
|
 |
Fig.
5. Donor site treated with transparent Comfeel (top picture) and aspect at day
six post-operatively (middle). A new, opaque dressing was applied, and maceration
developed (bottom picture). |
 |
 |
|
Another deisrable feature of this sort of
dressing is its action as a barrier against infection, which would prevent
epithelialization and even increase the defect. It has also been shown that an acid,
hypoxic microclimate reduces bacterial proliferation and enhances the leukocyte phagocytic
function (Mertz, Marshall and Eaglestem, 1985; Varghese and Balm, 1986).
An important point in the management of donor sites is pain, which often requires the use
of analgesics. Several authors have observed that the creation of a moist enviroment on
the wound considerably reduces the painful feeling (James and Watson, 1975; Barnett and
Berkowicz, 1983; Davies, 1984; Leicht, Slim and Sorensen, 1989). In our practice, we
consider this issue to be the most important to address.
Finally, dressings should be easy to manage with regard to changes, and the cost/benefit
relationship should be clearly shifted to the latter.
We have clearly obtained excellent results compared to our traditional dressing (used in
our Department for years) with the hydrocollold dressing, in two main aspects: reduced
epithelialization time and marked pain relied. In two recent papers (Leicht, Slim and
Sorensen, 1989; Hermans, 1990) very similar results with another hydrocolloid dressing are
reported. Fig. 4 shows the marked difference between both dressings on day 10. Tulle tends
to peel off the new skin because of its adherence to the wound.
The problem most widely reported with this sort of dressing is its detachment from the
donor site due to haemorrhage or fluid accumulation (Leicht, Slim and Sorensen, 1989).
Epinephrine appears to be fundamental to prevent oozing under the dressing. In fact we had
haematomas under five dressings, two on the buttocks and one on the abdomen, where
compression is very difficult to achieve. Should this complication happen, another
hydrocollold sheet should be applied after removal of the dressing, and cleansing of the
donor site.
The aspect of the dressing worsens as the days go by, because of accumulation of a thick,
creamy fluid underneath. Patients and nurse staff have to be warned about this, in order
to avoid confusion with pus. Even though this fluid build-up is normal, clinical infection
is very rare and accounted for only 2% oCour cases. The transparent dressing appears to
offer some advantages over the opaque one: better attachment to skin, less production of
fluid underneath, and closer follow-up of the donor site (Fig. 2).
We have noticed a trend towards skin maceration when the opaque dressing is kept on the
wound for longer than two weeks (more or less two dressing changes) (Fig. 5) since it
produces much more fluid accumulation than the transparent dressing. There is no doubt
about the enhanced growth of epithelium, but when used for a long period, excess of local
humidity may cause its loss.
We conclude that this new dressing is very satisfactory for donor site management because
it hastens epithelialization, it is very comfortable for the patient, and with careful
application very few dressing changes are needed. The cost of the dressing is slightly
higher but we think this minor drawback is outweighed by its advantages.
RÉSUMÉ. Les auteurs ont effectué une
épreuve du nouveau pansement Comfeeff' sur 100 sites donneurs de peau. Ils ont évalué
les paramètres suivants: temps d'épithélialisation, douleur, facilité d'emploi, et les
complications. Le Comfeel s'est montré très satisfaisant parce qu'il a réduit le temps
d'épithélialisation, il a été bien supporté par les patients, et il a nécessité peu
de changements du pansement. Ces avantages sont plus importants du coût légèrement plus
élevé.
BIBLIOGRAPHY
- Alvarez O.M., Mertz P.M., Eaglestein W.H.: The
effect of occlusive dressings on collagen synthesis and reepithelialization in superficial
wounds. J. Surg. Res., 35: 142, 1,983.
- Barnett A., Berkowiz R.L.: Comparison of synthetic
adhesive moisture vapor permeable and fine mesh gauze dressing for split thickness skin
graft donor sites. Am. J. Surg., 145: 379, 1983.
- Davies J.W.L: Synthetic materials for covering bum
wounds. Progress towards perfection. Part 1. Short term materials. Burns, 10: 94, 1984.
- Flermans M.H.E., Hermans R.P.: Duoderm and
alternative dressing for smaller burns. Burns, 12: 2 14, 1986.
- Hermans M.H.E.: Duoderm E in the treatment of donor
sites: a report. Annals of the MBC, 3: 166, 1990,
- Horikoshi T., Balin A.K., Carter D.M.: Effect of
oxygen on the growth of human epidermal keratinocytes. J. Invest. Dermatol., 86: 424,
1986.
- James J.H., Watson A.C.H.: The use of Opsite, a
vapour permeable dressing on skin graft donor sites. Br. J. Plast. Surg., 28: 107, 1975.
- Leicht P., Siim S., Sorensen B.: Treatment of donor
sites. Duoderm or Ormiderm? Bums, 15: 7, 1989.
- Linsky C.B., Roove D.T., Dow T.: Effect of dressing
on wound inflammation and scar tissue. In: Dineen P., flildick-Smith G. (Eds.): "The
surgical wound". Lea & Febiger, Philadelphia, 19 1, 1981.
- Mertz P.M., Marshall P.A., Eaglestein W.H.:
Occlusive wound dressings to prevent bacterial invasion and wound infection. J. Am. Acad.
Dermatol., 12: 662, 1985.
- Pollack S.V.: Wound healing: a review. 11.
Environmental factors affecting wound healing. J. Dermatol. Surg. Oncol., 5: 477, 1979.
- Queen C., Evans J.H., Gaylor J.D.S.: Burn wound
dressing - a review. Burns, 13: 218, 1987.
- Varghese M.C., Balin A.K.: Local environment of
chronic wound under synthetic dressings. Arch. Dermatol., 122: 52, 1986.
- Winter G.D.: Epidermal regeneration studied in the
domestic pig. In: Maibach HT, Roove D.T. (Eds.): 'Tpidermal wound healing". Year Book
Medical Publishers, Chicago, 71, 1972.
|