| Annals of the MBC - vol. 4 - n' 4 - December 1991
EVALUATION OF EMPIRICAL ANTIBIOTIC TREATMENT IN SEPSIS IN THE BURN PATIENT WITH CEPTAZIDIME-AMINOGLYCOSIDE ASSOCIATION Lenguas F., Herruzo R., Pintado R., Denia R., Mariscal F., Silva MJ. Critical Burns Unit, "La Paz" Hospital, Madrid, Spain SUMMARY. An empiric antibiotic treatment was made with th i rd-gene ration cephalosporins (ceptazidime-aminoglycoside), in 18 critical burns patients with clinical sepsis without bacteriological confirmation; the evaluation of plasmatic levels and M.I.C. (minimum inhibitory concentration) of ceptazidime was made. The successes and failures of the this dual antibiotic treatment, the high incidence of sepsis by Staphylococcus epidermidis in relation to Pseudomonas aerugmosa (20%), and the selection of resistances to aminoglycosides and beta-lactam antibiotics were discussed. We recommend treatment with aminoglycoside-vancomycin antibiotic in the case of existence of sepsis without bacteriological confirmation. Introduction The critical burns patient is one of the most serious in medical -surgical pathology, as he is a prototype of the immunosuppressed patient (Gelfand 1984), since equally the burn in itself, the numerous surgical operations, and the blood and plasma transfusions lead to a transitory secon arimmunodeficiency syndrome. There are there ore frequent septic complications which constitute, according to Curreri et al. (1980), the main cause of mortality, even though the local and systemic treatments are correct. The principal microorganisms which provoke these sepses are Staphyloccocus and Pseudomonas (MacMillan et al., 1986), and thirdly Enterobacteriaceae. For this reason an empiric treatment with aminoglycoside and third-generation cephalosporins was started, due to the good results obtained, according to several publications (Blint et al., 1983, Abbas et al., 1983, Wittman et al., 1981). Material and methods A) All the critical burns patients with a TBB surface > 40% and/or of electrical origin, with risk factors such as post-inhalation respiratory insufficiency, renal failure, existence of cardiopathy or pulmonary obstructive illness, and age over 65 or under 15 years, and who for these reasons were considered "high risk" on admission, were included. The number of patients with clinical sepsis (with or without later bacteriological confirmation) was 18, in the first 8 months of 1986. They were all admitted to the Critical Burns Unit of "La Paz" Hospital. The empiric treatment consisted of 2 gm of ceptazidime i.v. every 6 hours and an aminoglycoside (generally tobramycin) in conventional doses. The prospective study and the evaluation of the treatment were made considering a "success" to be the non-existence of micro-organisms in the blood on completion of treatment; "superinfectlon" the finding of new germs different from the original ones; and "failure" the persistence of the same micro-organisms responsible for the sepsis. B) M.I.C. (minimum inhibitory concentration) of ceptazidime against isolated micro-organisms. 64 micro-organisms isolated from critical care patients in 1985 were used: 18 Pseudomonas aeruginosa, 10 Staphylococcus aureus, 12 Escherichia coli or Proteus sp. and 24 S.E.K. group (Serratia, Enterobacter, Klebsiella). The M.I.C. was obtained by means of the introduction into Mueller-Hinton agar plates of ceptazedime in increasing concentrations (ratio: 2), from 0.5 to 128 microgr/ml The previous microorganisms, at a concentration of 10/ml, were inoculated in the plates by means of the Steers applicator, and the smallest concentration of anti-microbial agent which inhibited the bacterial growth in 48 hours was considered to be the M.I.C., as carried out in a previous work (Herruzo et al., 1985). In the same way two micro-organisms, Staphylococcus aurcus ATTCC 6538 and Pseudomonas aeruginosa ACC 15442, were used as a double check. C) Evaluation of ceptazidime levels in patients' plasma. This was done by microbiological method (Edberg and Sabath 1980) with a strain of Enterobacter cloacae resistant to aminoglycoside and susceptible to ceptazidime. Blood was extracted to determine these le vels half an hour before and after each of 6 doses of the antibiotic combination. 9 cases were analysed. The pattern concentrations and their zones of inhibition were introduced into a Mackintosh Plus computer for processing with the Cricket programme, which calculates the equation of regression between the variables and displays them graphically, allowing us to calculate the problem levels either by substituting the corresponding inhibition zone in the equation or by extrapolation of the zone from the graph. Results The characteristics of the 18 patients as well as their infections and evaluation of appropriate treatments are displayed in Table 1. The following facts are clear: Average age: 33.9 +/- 3.5 years
Negative blood culture post-treatment: 6
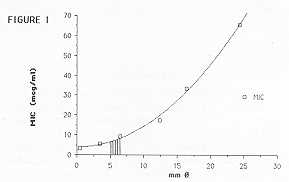
cases (33%) NOTE: The micro-organisms included in the "previous culture` concept were not known at the time of instigating the therapy because it is an empiric treatment. The M.I.C. of the 64 micro-organisms and its double-checking for ceptazidime are laid out in Table 11. M.I.C. 50 and M.I.C. 90 are distinguished by~dotted lines ( ... ) and ( --- ). It is noticeable that M.I.C. 50 is very low (<1 microgr/ml) in Staphyloccocus, E. coli and Proleus, low (<4 microgr/ml) in Pseudomonas, and moderate (<16 microgr/ml) in the K.E.S. group. M.I.C. 90 is high (-~128 and 64 microgr/ml respectively) in Staphylococcus and Pseudomonas, moderate (<16 microgr/ml) in the K.E.S. group, low (<8 microgr/ml) in E. coli and Proteus. Fig. I represents the curve-pattem and its corresponding equation in order to calculate the ceptazidime levels in burn patient plasma. The shaded area represents where the 9 cases are to be found: peak levels less than 4 microgr /ml in 8 of the 9 patients and 10 microgr/ml in the 9th. The "valley" levels were all less than 2 microgr/ml, undetectable by the microbiological method.
Discussion What stands out in this study is the
very low mortality in spite of the prediction of mortality on admission to the Unit. This
is due to the better treatment, both surgical and general, of critical burns patients,
compared to that given when the probit indexes were established in the Unit (197 1). Of
all the cases which constitute a success in empiric treatment, one was selected, P. aeruginosa
(non poly-R), in the digestive tract as a consequence of this treatment. Successes
were obtained in Enterobacter sp. or S. epidermidis sepsis (3 cases).
RÉSUMÉ. Nous avons effectué le traitement antibiotique empirique avec les céphalosporines de troisième génération (ceptazidime-aminoglycoside), chez 18 patients avec brûlures critiques qui présentaient une sepsis clinique sans confirmation bactériologique; l'évaluation des niveaux plasmatiques et de la M.I.C. (concentration inhibitrice minimum) de ceptazidime a été effectuée. Nous avons discuté les succès et les échecs de ce double traitement antibiotique, le taux élevé de sepsis par Staphylococcus epidcrmidis par rapport à Pseudomonas aeruginosa (20%), et la sélection des résistances aux aminoglycosides et aux bétalactamines. Nous recommandons le traitement avec l'antibiotique aminoglycoside-vancomycin dans le cas de la présence de sepsis sans confirmation bactériologique. BIBLIOGRAPHY
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||