| Annals of the MBC - vol. 4 - n' 4 - December 1991
THE TREATMENT OF TIBIAL OSTEOMYELITIS FOLLOWING BURN INJURIES Gabilondo F.J., Torrero J.V., Llop M. Department of Plastic Surgery and Burn Centre, Hospital Cruces, Baracaldo, Vizcaya, Spain SUMMARY. The tibial osteomyelitis, underlying ulcers of the lower third of the leg in serious bums cases poses, after survival of the acute episode, a two-sided problem: (i) the cleansing of the bone of the affected and isolated zone which is the cause and location of the osteomyelitis, resistant to conventional treatment, and (ii) the covering of the ulcer in a zone which with difficulty provides soft parts, aggravated by the fact that the extremities are covered with grafts in patients with bad cutaneous covering and few donor zones. This accumulation of circumstances can be resolved by providing a cutaneous covering of good quality with its own vascularization from another area which closes the defect, not only of the ulcer but also of the larger zone of the cleansing of the bone in the alIceted area. To do this, we used a free skin flap with its vascular pedicle connected to the posterior tibial artery outside the zone of the pathology. Introduction In cases of extensive burns whose
gravity requires a large quantity of self-grafts to cover the zones with deep burn which
have been previously removed, one must propose a second stage in their treatment with
reconstruction problems which are difficult to resolve in patients with large areas of
grafts. One of these problems is the presence of ulcers in the inferior extremities with
bone involvement in the inferior third of the tibia, with exposed bone and episodes of
underlying osteomyelitis. The solutions of this problem using techniques with neighbouring
tissues, or using the other extremity which is also burned, are not fully appropriate to
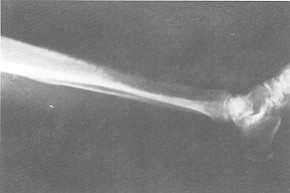
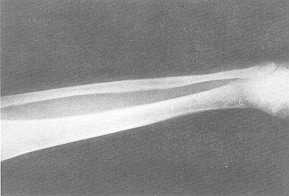
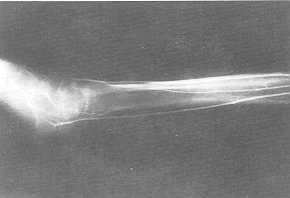
the therapeutic requirements. This is true of the case with which we are concerned, whose
previous state can be seen in the figures (1, 2, 3). Discussion and commentary Osteomyelitis of the lower third of the tibia poses a challenge in its treatment which demands various aims: resection of the osteomyelitic zone of the bone,
It is better to perform the vascular
anastomosis as far as possible from, and in a proximal sense to, the zone of the
pathology, as was done in the posterior tibial artery in a proximal sense for greater
security. All this is possible with the free forearm skin flap chosen, if its vascular
pedicle has considerable length and good size vessels.
a covering with good vascularization and,
in the case of patients with burns in both inferior extremities, the limited possibility
of other traditional procedures such as cross-leg grafts, neighbouring flaps re-covered
with grafts or muscular flaps in badly affected extremities and in a serious condition.
RÉSUMÉ. L'ostéomyélite tibiale sous-jacente aux ulcères du tiers inférieur de la jambe dans les cas de brûlures sévères pose, après le moment aigu, un problème qui peut être appréhendé de deux façons: (i) le nettoyage de l'os dans la zone atteinte et isolée qui est la cause et.la localisation de l'ostéonryélite, résistante au traitement conventionnel, et (ii) la couverture de l'ulcère dans une zone qui offre peu de parties molles, ce qui est aggravé par le fait que les extrémités sont couvertes de greffes en des patients ayant une mauvaise couverture cutanée et peu de sites donneurs. Cette combination de circonstances peut être résolue en créant une couverture cutanée de bonne qualité avec sa propre vascularisation provenante d'une autre zone qui ferme le défaut non seulement de l'ulcère mais aussi de la zone plus grande du nettoyage de l'os dans la zone atteinte. Pour faire cela, nous avons utilisé un lambeau libre de peau avec le pédicule vasculaire relié à l'artère tibiale postérieure hors de la zone pathologique. BIBLIOGRAPHY
|