| Annals oj'the MBC - vol. 4 - n' 4 - December 1991
TUMOURS OF THE UPPER LIMB AND BURN SCARS. CASE REPORTS Napoli B., D'Arpa N., Conte F., Masellis M. Divisione di Chirurgia Plastica e Terapia delle Ustioni, Ospedale Civico, U.S.L. 58, Palermo, Italia SUMMARY. After a brief description of the actiopathogenesis of carcinoma occurring in burn scars, some such cases are presented that were observed in the upper limb. It is concluded that these tumours can be avoided by preventive treatment of unstable scars. Introduction Skin carcinoma, of both basocellular and 1
spinocellular form, can develop in scar tumour. In particular, it may occur in a burn scar
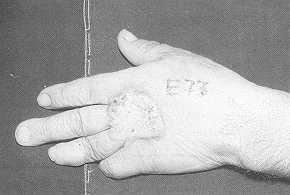
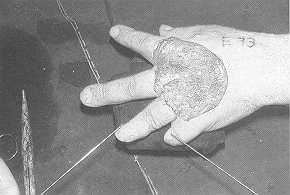
(Marjolin's ulcer) (2, 4). Case reports Between 1975 and 1990 we treated 37 cases of epithelloma in the upper limb, 13 of which (35.13%) were basallomas and 24 (64.87%) spinallomas. Of the latter, 6 (25%) occurred in burn scars, 2 (8.33%) in other lesions (trauma, actinic keratosis), while in the remaining 16 cases (66.67%) no precise anamnestle data were available. Case 1 M.G., male, age 62 years, admitted in September 1983 with the diagnosis of "recidivation of neoplasia in burn sequela in dorsal lower third left forearm", presented with a walnut-sized vegetating-ulcerated neoformation. Anamnesis revealed that the burn occurred in the patient's childhood. In November 1974, in another hospital, he was subjected to exeresis of a neoformation in a burn scar on the left elbow. This was followed by the onset of a torpid ulcer which in June 1975, in our Department, was covered by an abdominal flap. In 1982 the patient presented with an onset of ulceration (histological tests showed a spinocellular epithelloma of medium-grade differentiation) in the left forearm, which was subjected to extensive excision and free skin graft. Recidivation, after one year, was not accompanied by clinically positive regional lymph nodes and it was retreated, under narcosis, with ample excision of the tumour and covering by a free skin graft obtained with a Padgett dermotome. Histological tests indicated a spinocellular, well differentiated, keratinizing epithelloma which totally infiltrated the fragment examined. The patient was therefore sent for radiotherapy. Since the therapeutic treatments he has not presented further local recidivations or lymph node metastases (Figs. I a, b, c). Case 2 M.S., mate, age 54 years, admitted in May 1983 with the diagnosis of "neoformation on the dorsal surface of the left hand occurring in a burn scar", presented with a vegetating neoplasia about 2 x 2 cm in size. Anamnesis revealed that the neoformation initiated ten years after the bum. On admission there was no clinical evidence of metastatic regional lymph node involvement. The surgical operation, under narcosis, consisted of an ample excision of the tumour with covering by means of free skin graft. Histological tests revealed a mature spinocellular carcinoma (Broders 1) and the poles and fundus of the resected part were unaffected. The patient did not have local recidivations or metastases becoming evident following removal of the tumour (Figs. 2a, b).
Case 3 S.G., male, age 65 years, was admitted in November 1983 with the diagnosis of "ulcerated neoformation in a burn sequela on the dorsal surface of the right hand". Anamnesis indicated a bum sustained at the age of 2 years, with a latency therefore of 63 years before appearance of the tumour. On admission the patient did not present lymph gland involvement. The tumour was removed, under narcosis, with ample excision, and covering was by free skin graft. Histological tests indicated a differentiated spinocellular carcinoma (Broders 11). The margins of the resected part were free of neoplasia. The patient had no local recidivation or lymph node metastases following the operation. Case 4 M.F., male, age 72 years, admitted in August 1987 with the diagnosis of "neoformation in a burn sequela in the left hand-, presented with an ulcerated neoplasia 2.5 x 2.5 em in size. The burn had been sustained some 40 years previously. The patient did not present palpable lymph nodes and the tumour was amply removed under narcosis. The bloody area was covered with free skin graft. Histological tests indicated a mature spinocellular carcinoma (Broders 1). The poles and fundus of the resected part were unaffected. The patient did not subsequently present recidivation or lymph node metastases. Case 5 B.V., male, age 60 years, was admitted in November 1987 with the diagnosis of -neoformation in a burn scar in the dorsal surface of the right handand presented with a vegetating neoplasia sized 12 x 4 em. It was not stated when exactly the burn occurred. There was no lymph node involvement and the operation, under narcosis, consisted of an ample excision of the tumour and covering by means of free skin graft. Histological tests indicated a mature spinocellular epithelioma (Broders 1) and the margins of the resected part were not affected by neoplasia. The patient did not present recidivation or lymph node metastases following the operation. Case 6 C.P.G., male, age 51 years, admitted in July 1989 with the diagnosis of "neoformation in a burn scar in the fold of the left elbow", presented with an ulcerated abscessed neoplasia the size of a walnut. Anamnesis indicated that the burn, caused by tar, had been sustained 10 years previously and that since then the residual scar had suffered various ulcerative episodes treated with unspecified medical therapy. In the absence of clinically appreciable lymph nodes, the operation consisted, under narcosis, of an ample excision as far as the fascia, followed by covering with free skin graft. Histological examination revealed a well-differentiated spinocellular carcinoma, with poles and fundus of the resected part unaffected by infiltration. So far the patient, since the operation, has not presented recidivation or lymph node metastases. Conclusion According to Dufourmentel (3), carcinomas developing in an unstable scar have the following three characteristics:
Surgical treatment of the tumour, when
already present, must therefore be performed in good time; early therapy can lead to
complete and permanent recovery. Removal of the regional lymph nodes, if clinically
positive, offers only limited survival. Results obtained with prophylactic lymphadenectomy
have also proved to be no longer encouraging (5, 7).
RÉSUMÉ. Les auteurs, après avoir décrit brièvement l'étiopathologie des carcinomes qui se produisent sur les cicatrices par brûlure, présentent les cas qu'ils ont observés à niveau du membre supérieur, en concluant que ces tumeurs peuvent être évitées par moyen du traitement préventif des cicatrices instables. BIBLIOGRAPHY
|