| Annals ofthe MBC - vol. 4 - n' 4 - December 1991
TWO SEVERE FACIAL BURN SCAR PATIENTS WITH LAGOPHTHALMOS LEFT
UNTREATED OVER A LONG PERIOD OF TIME
Yano K., Hata Y.
Department of Plastic Surgery, Kagawa Medical School,
Japan
SUMMARY. Two cases are described
of patients with bum lagophthalmos left untreated for a long period. Skin grafting was
performed in both cases and the results are described.
Introduction
The skin of the eyelid is thin and the
eyelids consist of loosely attached tissues. They are therefore readily submitted to the
pull of contracting healed burned tissues over the periphery of the orbital rims.
Cicatricial lagophthalmos caused by ectropion is associated with many pathological
conditions such as excessive tear production, conjunctivitis, keratitis, comeal ulcer and
perforation.
We performed skin grafting in 2 patients with burn lagophthalmos left untreated for a long
period and observed improvement in visual acuity. Changes in the eyeball and facial
morphology are reported during the course of treatment.
Case 1
The patient was a 41-year-old woman who
suffered burns at the age of 8 months when she fell into a brazier with her face directly
exposed to the fire. At that time she received first-aid treatment from a doctor in the
neighbourhood. At the age of 19 years, she received skin grafts to both upper eyelids and
the corners of the mouth. However her lagophthalmos hardly improved, and it had never been
properly treated over the past 20 years. She always suffered from excessive tear
production and the sensation of a membrane over the corneas. More recently she also
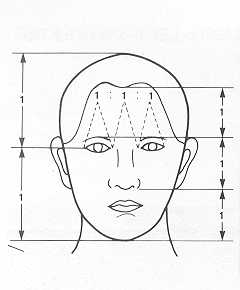
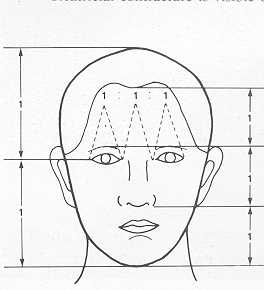
complained of ophthalmalgia. Bum contracture is visible over her whole face (Fig. 1). By
reference to Leonard's ratios of the face, it is noticeable that her face is
longitudinally narrowed in the upper two thirds (Fig. 2).
 |
Fig. 1 Case
1. Pre-operative view. Burn contracture is visible over the whole face. |
|
|
|
Fig.
2 Leonard's ratios of Case 1. Longitudinal narrowing in the upper two thirds is
noticed. |
|
A cephalogram shows a normal range. It is
remarkable that her lagophthalmos remains as can be seen by comparing the situation with
eyelids open and closed (Fig. 3).
Measurements of the eyes indicate larger vertical values and smaller horizontal values for
the palpebral fissure, whether the eyelids are open or closed.
Because of the larger slope of the palpebral fissure for both eyes, it is noticeable that
the face is stretched towards the centre, i.e. towards the nose (Fig. 4).
 |
 |
| Fig.
3 Lagophthalmos with eyelids open and closed. |
|
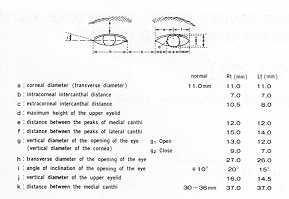 |
Fig. 4 Measurements
of the eyes of Case 1. |
|
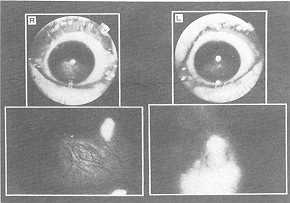
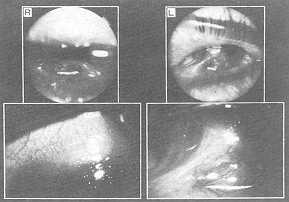
The condition of the eyeballs shows prominent clouding and
pannus extending to the pupillary zone in the right cornea. Clouding is also noticeable in
the left cornea, but there is no prominent pannus (Fig. 5).
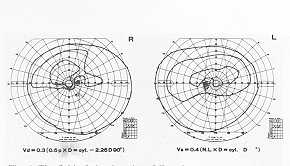
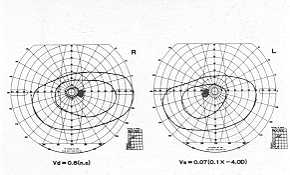
An eye-fundus picture shows no remarkable change in either eye. Visual acuity is low in
both eyes. Vision is affected at the lower field in both eyes but more strongly in the
right (Fig. 6).
 |
 |
| Fig. 5 The
condition of the eyeballs of Case 1. |
Fig. 6 The
field of visual acuity of Case 1. |
|
Examination of the lacrimal function by
Silmer's Test demonstrated the function to be within normal range.
The patient received a skin graft to the upper right eyelid in July 1985. According to the
operative findings, both eyelids had thick scar, and the traces of orbicularis ocull and
rolled tarsus were found. Levator muscle function was normal. After the whole scar was
excised, skin graft was performed with zigzag incision in the vertical lesion along the
aesthetic unit. In 1990, both eyebrows were reconstructed using arterial island scalp
flap. The patients has been showing favourable progress since then (Fig. 7).
 |
 |
| Fig. 7 The
post-operative condition of Case 1. |
Fig. 8 Case
2. Pre-operative view. Cicatricial contracture is visible over the whole face. |
|
The patient now feels more at ease with
both eyes. Acuity has improved from 0.3 to 0.6 in her right eye, and from 0.4 to 0.7 in
her left eye after one year.
Case 2
The patient was a 66-year-old man who visited the
ophthalmological department of our hospital hoping to receive an operation for pterygoid
fragments, but was referred to our department for correction of lagophthalmos. The present
condition began 43 years ago when he suffered bums in a plane crash during the Second
World War. After the ulcer had healed, he received skin grafts to the face and right hand
in 1971, and to the face and left hand in 1980 at another clinic. However his
lagophthalmos remained unchanged for about 40 years, and recently he had begun to complain
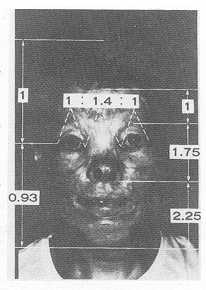
of photophobia and reduced visual acuity. His facial condition is characterized by the
presence of cicatricial contracture over the whole face (Fig. 8).
Lconard's ratios indicated narrowing in the upper two thirds (Fig. 9).
 |
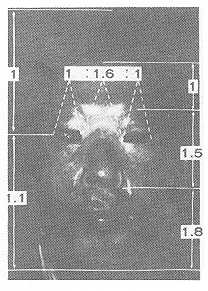 |
| Fig.
9 Leonard's ratios of Case 2. |
|
A cephalogram was within normal range. It is noticeable
that the lagophthalmos remains, as can be seen comparing the situation with eyelids open
and closed (Fig. 10). Measurements of the eyes demonstrate shorter than normal horizontal
and vertical lengths of the palpebral fissure in both eyes. The narrowing of the palpebral
fissure is quite noticeable. Even with the eyes closed, there are 2 min of
lagophthalmos.The eyeballs indicate the presence of pterygoid fragments in both eyes,
together with corneal clouding and parmus, although this does not reach the pupillary zone
(Fig. 11).
 |
 |
| Fig.
10 Lagophthalmos with eyelids open and closed. |
|
 |
 |
| Fig. 11 The
condition of the eyeballs of Case 2. |
Fig. 12
The field of visual acuity of Case 2. |
|
An eye-fundus picture shows no remarkable
change in either eye. Visual acuity is reduced in both eyes, but the upper field of vision
is affected because of contracture in both eyelids (Fig. 12). The patient's lacrimal
function, examined by Silmer's Test, was found to be within normal range, but the patient
has always suffered from excessive tear production.
The patient received skin grafts to the upper eyelids of both eyes in January 1985. The
operative findings were almost the same as in Case 1. After the whole scar was excised,
skin graft was performed with zlgzag incision in the vertical lesion along the aesthetic
unit. In 1990, both eyebrows were repaired using scalp flap as in Case 1. Acuity has
improved from 0.4 to 0.7 in the left eye, and right eye acuity was the same after one
year. The patient has been showing favourable progress (Fig. 13).
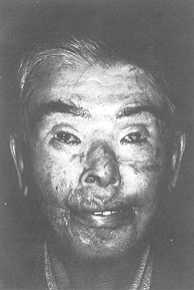 |
Fig. 13
The post-operative condition of Case 2. |
|
Discussion
Visual impairment associated with
facial burns is due to direct or indirect ocular damage.
Direct ocular damage is injury to the cornea by burns themselves while indirect ocular
damage is caused most frequently by lagophthalmos following burns on the eyelid.
Schofield (8) classified facial burns according to causes and found direct ocular damage
in 14.5% of patients with flash and flame burns and 49% of those with fire burns. He
reported that facial burns were frequently observed in children, who are slow in their
movements, and in unconscious people. In our study, patient I was an infant with facial
burns and patient 2 had bums all over the body. It is highly likely that their eyeballs
suffered some direct injury by the burns at that time.
The treatment of facial burns in the acute phase, whether or not burns have directly
injured the eyeball and cornea, must first be determined. When the possibility of foreign
body aberration in the eye cannot be excluded, the patient should be promptly referred to
an opthalmologist (4, 5). If this is delayed, hydroblepharon progresses, and the eyes
cannot be opened, which impedes sufficient ocular examination. If the eyelid is already
swollen, it is important to te 11 the patient that it will subside spontaneously in 3 to 4
days.
The ocular damage associated with burns sometimes seems to involve not only the comea but
also the iris, lens and other parts.
This is supported by the report by McIndoe (6) who found no improvement in patients with
blindness due to bums who underwent corneal grafting. Damage in the eyeball should
therefore be treated as early as possible to prevent progression of the damage.
However, in our patients, the most common cause of visual damage was lagophthalmos left
untreated for a long period.
It is well known that elcatricial lagophthalmos induces lacrimation, conjunctivitis,
keratitis, comeal ulcer and perforation of the comea.
It is surprising that our patient with advanced lagophthalmos who was left untreated for
40 years did not suffer from complete blindness. It was probably because his lacrimal
function remained normal, and the inverted conjunctiva protected part of the cornea. In
addition to the above-mentioned direct and indirect cause, visual damage was reported to
be caused by shielding of the eyeball in hospital (2, 3, 8). Visual damage may occur when
the eyes of infants and children with facial bums are covered with occlusive dressings and
are shielded from light.
According to Awaya (1), who reported ---amblyopla due to blockage of optic
stimulation", a decrease in the optic function is not likely to occur when both eyes
are occluded, but it may appear when only one eye is occluded even for as little as a
week.
When the two eyes are occluded at different times, the second one develops amblyopia. The
term for the stage when these changes become irreversible is the "critical
period", which is about one year of age in humans. Avoidance of the occlusive
dressing technique therefore is most important for the prevention of amblyopia. When
occlusion cannot be avoided due to swelling of the eyelid in patients at the acute stage,
light stimulation should be given at regular intervals. The patient in Case 2 was treated
by this technique for one week and the possibility of amblyopla occurring cannot be
excluded.
The association of lagophthalmos due to contracture poses a problem in burns of the
eyelid. To prevent this condition, skin grafting is the procedure of first choice, for
which two proceeding techniques are available: (1) relief incision and (2) removal of the
entire scar of the eyelid along the aesthetic unit (7). When only a relief incision is
used, the residual scar shows excessive folds around the eye. In addition to this
shortcoming, the difference in colour tone between the cicatricial area and the skin graft
becomes clear, posing an aesthetic problem. In skin grafting of the upper and lower
eyelid, we therefore think it best to resect the entire cicatricial tissue along the
aesthetic unit. The area behind the ear is the donor site of first choice from the
standpoint of the properties, colour tone and touch of the blepharal skin as in Case 2.
When this skin graft is not available, we collect a graft from the medial area of the
forearm, as in Case 1.
Since it is essential to prevent lagophthalmos and to protect the comea, temporary bedside
tarsorrhaphy is recommended for patients whose general condition does not permit skin
grafting. If surgical treatment results in successful opening of the eye in a patient with
lagophthalmos, such as our patient, who was left untreated over a long period, functional
and morphological repair seems to some extent possible.
Regarding morphology after severe facial burns, it is characteristic that the face is
stretched towards the centre, i.e. towards the nose.
RÉSUMÉ. Les auteurs décrivent deux cas de
patients atteints de lagophthalmie causée par des brûlures qui est restée sans aucun
traitement pour de longues périodes. Dans tous les deux cas la greffe de peau a été
effectuée et les résultats sont décrits.
BIBLIOGRAPHY
- Awaya S., Miyake Y., Kanda T. et al.: Further
studies on cases of suspected stimulus deprivation amblyopia. Jap. J. Ophthalm., 25:
270-28 1. 1974.
- Converse J.M.: "Reconstructive plastic
surgery", Second ed., W.B. Saunders Co., Philadelphia, London, Toronto, 1977.
- Gonzalez-Ulloa M.: Restoration of the face covering
by means of selected skin regional aesthetic units. Br. J. Plast. Surg., 9: 2 12-221,
1956.
- Grant W.M.: Action of alkalis on the corneal stroma.
Arch. Ophth., 54: 93 1-939, 1955.
- Hughs W.F.: Alkali burns of the eye. Arch.
Ophthalmol., 35: 423, 1949.
- Mclndoe A.H.: Total reconstruction of the burned
face. The Brads How Lecture 1958, Br. J. Plast. Surg., 36: 410-420, 1983.
- Namda K., Horiuchi H.: Treatment of burned face.
Traumatology, 8: 112, 1977.
- Schofield A.L.: A review of bums of the eyelids and
their treatment. Br. J. Plast. Surg., 7: 67-91, 1954.
|