| Annals qf the MBC - vol. 5 - n* 1 - March 1992
EPIDEMIOLOGY AND PREVENTION OF BURNS AT
GERIATRIC AGE
D'Arpa N., Napoli B., Masellis M.
Divisione di Chirurgia Plastica e Terapia
delle Ustioni, Ospedale Civico, USL 58, Palermo, Italia
SUMMARY. With
a view to prevention, an investigation was made of the circumstances, the modalities and
the lesive agents responsible for burns to elderly patients admitted to hospital during
the period 1975-1991. The factors to be considered in the preparation of a prevention
campaign are indicated and suggestions are given as to how the campaign can be developed.
Introduction
Dorland's Illustrated Medical Dictionary defines geriatrics (from the Greek geras =
ageing and iatrike = medicine) as the branch of medicine that deals with the
problems of old age and ageing, including the clinical problems of senescence and
senility.
The term "geriatric" therefore refers to everything that is pertinent to the
treatment of persons of advanced age. However, with the extension of the mean lifespan in
recent decades, advanced age now has wider parameters. It is therefore possible to come
upon elderly persons still actively occupied who have passed the age of 65 years, the
minimum age in Italy for retirement.
For these reasons the minimum age-limit of 65 years does not correspond with actual
physical incapacity, and this accounts for the presence among our case histories of burns
occurring in places of work. It must also be added that any work carried out without the
security guarantees required by the law increases the risk of accidents.
In the period 1975-1991, 230 burned persons of geriatric age were admitted to the
Department of Plastic Surgery and Burns Therapy at Palermo Civic Hospital, 114 of whom
(49.5%) in the last 6 years.
The progressive ageing of the population, which is without any doubt responsible for the
increase over the years in the burns rate among the elderly, draws our attention to the
problem of the prevention of such burns.
Central to this is an investigation of the circumstances, the modalities and the lesive
agents involved in burns of the elderly, not neglecting the presence of pre-existing
diseases which by the disabilities they cause may have been directly responsible for the
burn accident.
Material and methods
The personal details of each patient were taken from the admission files (age, sex, place
of origin); the same was done for athologies existing prior to the burns and for the
dynamics of the accident. In the absence of witnesses of the accident, the information in
the anamneses was in some cases incomplete, owing to the patients' advanced age or their
very severe clinical condition on admission.
Despite these limitations, which are characteristic of any retrospective investigation
based on written records, we were able to collect sufficient material for our inquiry.
Analysis of the data
Regarding age, the patients were subdivided into groups, within which they were
distinguished by sex. There was no appreciable sex prevalence and the percentage of
patients in each age-group reduced progressively after the age of 75 years (Fig. 1).
As for place of origin (Fig. 2), the majority of patients (69.2%) were from Palermo and
its province, the remainder coming from the other Sicilian provinces (26.9%) and from
outside the island (3.9%).
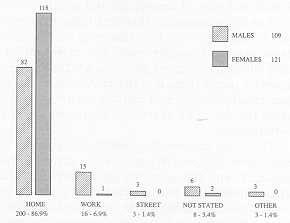
The highest percentage of accidents occurred in the home (86.9%) (Fig. 3); considering
only females, this percentage rose to 98.3%.
Burns occurring during work activity accounted for 16 cases (6.9%); 15 of these (14 males,
1 female) were caused by burning stubble or dry grass in the country; in one case a
shepherd burned himself with whey while making ricotta.
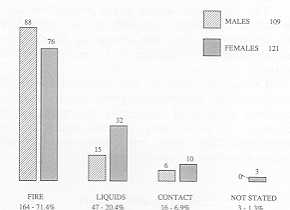
The lesive agents were distinguished as follows. fire, liquids, contact, not stated (Fig.
4). Among these elderly patients the main cause of burns was fire (71.4%), including those
caused by the use of flammable liquids (surgical spirit, petrol). Out of the 47 cases
(20.4%) of burns due to liquids (hot tomato sauce, oil, heated wine, whey, water) 42
(18.2%) were caused by boiling water.
Of the 16 contact burns (6.9%) 1 was caused by an engine-silencer, following a road
accident, 3 (1.3%) by an electric blanket, and 1~ (5.2%) by falls on to electric fires.
There were no cases of chemical or electrical burns.
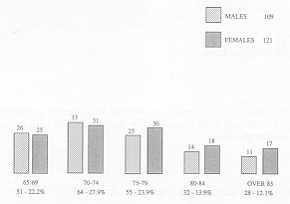 |
Fig. I Age/sex
distribution. |
|
As the list of lesive agents did not
provide complete information for the purposes of the research, attention was directed to
the modalities of the burn accidents.
 |
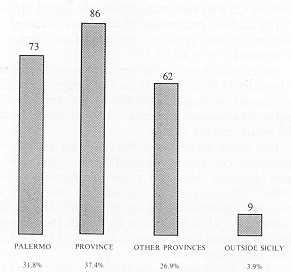 |
| Fig.
2 Distribution by place of origin. |
|
Fire burns
In 44 cases (26.8%) the burn was caused by flares or fires or explosions due to gas leaks
from malfunctioning gas bottles in kitchen cookers or heating appliances. The improper
functioning of commonly used articles, generally in the home, is the pre-condition of such
accidents, which are then triggered by a match being struck, the light being switched on,
or by the spark caused by a short-circuit.
 |
 |
| Fig. 3 Distribution
by place of accident. |
Fig. 4 Distribution
by lesive agents. |
|
Second in frequency are burns caused by
sudden violent flares caused by using flammable liquids such as surgical spirit and petrol
to liven up the fire in a hearth, barbecue, etc. Carelessness, rashness and ignorance play
a fundamental role in this type of burn, of which there were 35 cases in our survey
(21.3%).The same mechanisms (carelessness, rashness, ignorance) were responsible for:
- burns occurring during the burning of stubble or dry grass
in fields (15 cases, equal to 9.1%);
- burns caused by the explosion of gas lamps during changing
of the cylinder in the proximity of a lighted candle or by the explosion of containers of
flammable liquids kept too near sources of heat (4 cases, equal to 2.4%);
- burns caused by using surgical spirit for medical dressings
while smoking a cigarette (2 cases, equal to 1.2%);
- burns caused by fires due to candles being forgotten alight
(2 cases, equal to 1.2%).
A large number of burns (22 cases, equal
to 13.4%) were the consequence of falls on to braziers or fireplaces and of clothing
catching fire, as a result of being too near a source of heat. Even if this modality of
burn accident is related to the practice in our population of using open and therefore
risky sources of heat, only a few such accidents were attributable to carelessness. The
anamnestic data showed that out of the 22 cases examined in at least 5 (3.0%) the direct
cause responsible for the accident was a form of incapacity (hypertensive seizure,
incapacitating sequelae of cerebral ictus). The same applies in the 13 cases (7.9%) in
which the burn was caused by mattresses or blankets catching fire while the patient was
smoking in bed or in an armchair. The accident was due to the patient falling asleep in
only 3 cases (1.8%), while in the other 10 (6.0%) serious disabilities were involved which
prevented all movement after the falling of a burning match, after the lighting of a
cigarette or pipe, had caused the fire (gangrene of the lower limbs, neoplasia,
incapacitating sequelae of cerebral ictus, blindness, acute alcoholism).
In 23 cases (14.0%) the pathogenesis was unstated or various. Two cases (1.2%) occurred as
a result of road accidents when the vehicle the patient was travelling in caught fire, and
in 2 cases (1.2%) the burns were due to acts of self-aggression (attempted suicide using
flammable liquids).
Burns due to boiling water
In 28 cases (66.6%) either the anamnesis was unstated or the burn modalities were various
(burns during vapour inhalation, ursting of hot-water bottle, breakage of flexible hot
water tubing in washbasin, etc.). In such cases carelessness and the malfunctioning of
everyday objects played a very important role. Six housewives (14.2%) were burned because
of the upsetting of pots of boiling water standing on top of the cooker or being carried,
when for example the h , andles came off. Eight persons (19.0%) were burned in the
bathroom either by falling into a bath of water or while showering, using the bidet or
washing their feet; the anamnesis showed that the fall into the bath was due in 3 cases to
a specific disability (Parkinson's disease, epilepsy, incapacitating sequelae of cerebral
ictus).
Contact burns
Of the 16 cases of contact burns we have already seen that 12 (75%) were due to falls on
to electric fires. All these cases involved a grave disability (sequelae of cerebral
ictus, epilepsy, Parkinson's disease, obliterating arteriopathy of the lower limbs).
Conclusions
Burns in the elderly represent a very serious problem, for two fundamental reasons:
- elderly patients generally suffer from one or more
pathologies, and this causes complex clinical and therapeutic problems;
- the I ife -endangering nature of burns cannot be
underestimated in elderly patients.
For these reasons prevention becomes a
matter of primary importance, and the formulation of a campaign of prevention must take
into account a series of factors which, as in the work of other authors, have been
highlighted in our research:
- carelessness, rashness and inaccurate assessment of
possible risks, all of which play an important role among the elderly;
- the possible existence of acute or incapacitating
disabilities;
- the misuse, whether deliberate or accidental, of objects
and instruments with which elderly people come into contact every day;
- acts of self-aggression;
- the frequency of accidental traumatic events involving the
elderly, as a result of the reduction of their capacity to react.
The campaign must be developed along very
well-defined guidelines:
- information courses to be held wherever the elderly
congregate (clubs, churches, rest homes, etc.);
- the adaptation of certain parts of the home to their
particular physical capacity, for example by fitting special support systems in the bath,
re-locating cooking areas away from cramped corners or passageways, recommending the use
of automatic air extraction systems in rooms where gas-leaks may the fitting of automatic
devices that automatically switch off electric household appliances if not used according
to instructions;
- specific surveillance and assistance of elderly people who
are incapacitated, depressed, alcoholic or who live alone.
RESUME. Les auteurs,
dans le but de la pr&vention, ont analysé les milieux, les modalités et les agents
lésifs responsables des brOlures chez les patients dg&s observ&s pendant la
période 1975-199 1 et traités dans leur Centre. Us incliquent les facteurs qui doivent
etre considérés dans la préparation des programmes de prévention et ils proposent les
modalités pour qu'ils soient développés.
BIBLIOGRAPHY
- Baldoni E.: "L'assistenza geriatrica, concetti
e tecniche di prevenzione e di recupero---, Piccin, Padova, 1986.
- Barisoni D.: "Le ustioni e il loro trattamento---,
Piccin, Padova, 1984.
- Baux S., Minoun H., Saade H., Lioret N., Esteve M., Nolland
X.B., Berti&re M.N.: Burns in the elderly. Burns, 15: 239-240, 1989.
- Dorland's Illustrated Medical Dictionary" (Ist),
Saunders, Philadelphia, 1985.
- Gilardino P., Peri A., Ronchi A., Donati L.: Epidemiologia
e prevenzione delle ustioni: esperienze a confronto. Riv. It. Chir. Plas., 22: 79-101,
1990.
- Scatafassi S.: Burn prevention. Organization of information
as a special service. Riv. It. Chir. Plas., 13: 253-258, 1981.
- Turner D.G., Leman C.J., Jordan M.11: Cooking-related burn
injuries in the elderly. J. Burn Care Rehabil., 10: 356-359, 1989.
|