| Annals of the MBC - vol. 5 - n' 1 - March 1992
BURNS IN CHILDHOOD - A TEN-YEAR EXPERIENCE IN
MANAGEMENT
Tryfonas G., Gavopoulos S., Limas C.,
Z¡outis l., Violaki A., Klokkaris A., Fragos E., Grigoriadis G.
Hippokration General Hospital, Pediatric
Surgical Clinic, Thessaloniki, Greece
SUMMARY. During the period from
1981-1990, 281 patients were hospitalized in our clinic, 174 males and 107 females. The
age ranged from 2 days to 14 years. In 72% of cases the bums were of second degree and in
28% they were of third degree. The patients were divided into two groups, according to age
and burned area. The method of choice was the undressed one. Autografts were used in 76
cases. Homografts, after histocompatibility determination, were used in 4 cases because of
the extensive burned area (60-75%). There were 3 deaths and the mean in-patient time was
28 days.
Introduction
Thermal trauma is second only to car accidents as a cause of death during childhood (1)
and it is a very common manifestation in child abuse (2). The majority of cases occur
indoors and the main causes in children under the third year of age are hot liquids,
especially water, and contact with electrical appliances; in older children flames are the
main cause. Since children do not tolerate thermal injury as well as adults, we have to
pay special attention to management in order to prevent mortality and to achieve a good
functional and cosmetic result.
Material and method
During the last decade 1725 burned children were examined in the emergency department of
our clinic and 281 of them were admitted. We used as guides the burned area, the depth
(although difficult in assessment at an early stage), the place of burn and, of course,
the age.
The classification of burns is shown in Table 1.
Patients with moderate or critical burns and those aged less than two years old were
admitted. There were 174 boys and 107 girls and the age ranged from two days to 14 years.
|
Second
degree |
Third degree |
Minor |
10% |
2% |
Moderate |
10-20% |
2-5% |
* Critical |
20% |
5% |
|
Table I Classification
of burns |
|
Burns involving
hands, face or feet were classified as critical (Munster A.M., 1980).
The majority of them were less than 6 years old (219), with a peak in the second year of
life. The burned area was less than 20% in most of them. The depth was assessed as
second-degree in 201 patients and third-degree in the rest.
The first aim of treatment was resuscitation with intravenous fluid administration.
Brooke's formula was employed, but it was modified under specific circumstances. The
undressed method was the method of choice except when joints and hands were involved, and
all patients were nursed in a special ward under invariable conditions of temperature and
humidity.
A daily programme was followed with cleansing and the spraying of povidone iodine in
droplets. This way of treatment was continued until the burn healed spontaneously or was
prepared for grafting by the third week.
In 201 patients who were conservatively treated the burned area ranged from 5% to 30% and
the mean in-patient time was I I days. Grafting was needed in 77 patients, as a result of
the initial depth or secondary to infections. The burned area mostly ranged between 5 and
35%, although in four cases the burned area covered 60 to 75% (Fig. 1). The mean
hospitalization time was 42 days. Autografts were used in all but four patients. In these
patients homografts were needed as a result of the extensive burned area and the mother
was the donor, after histocompatibility determination.
Results
Five children presented rejections of the grafts due to infections or inappropriate
technique. Infections were also the main causes for partial rejections that did not
necessitate any further treatment. Hypertrophic scars in 12 patients and dysfunction in 18
were the main problems we faced.
 |
Fig. I
Ten-year-old boy after conflagration with spirit. The burned area was estimated at 65%. |
|
All patients with functional problems were
treated surgically. The patients with hypertrophic scars were initially treated
conservatively by applying cortisone cream and compressive dressing. This treatment was
successful in all but five children, who eventually underwent surgical excision and
grafting. Three children with extensive deep bums died, as a result of resuscitation
failure in two cases and sepsis in one.
Discussion
The proper treatment of burns has been the subject of debate and intense research for
several years, and the safest and most acceptable method is still controversial. Leaving
the burns uncovered is a well-established treatment in many centres. We employ this
method, except when a joint or hand is burned, in which case we cover the burned area and
change the dressing every three days. The daily programme with cleansing is used in all
patients but if the burned area is extensive the patient has a daily bath in a special
apparatus. Homografts, which were received from a related donor, such as the mother, after
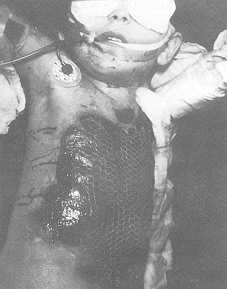
histocompatibility determination, and autografts were used as mesh grafts (Fig. 2, 3). We
think that there are two main advantages in employing mesh grafts. It is easier to cover
an extensive burned area with a small graft and drainage is easier. Many other methods
have been suggested, such as allografts (4), xenografts (5), early excision (6), and the
abrasion method (7), in the attempt to achieve the most successful treatment. Good results
have been referred by the researchers of these methods. Our experience is somewhat limited
because we did not early excision and grafting in the near future aims at employ these
methods, as our results were satisfactory reduction of hospitalization stay, as mortality
is using the undressed one. Our intention to employ insignificant in our series.
 |
 |
| Fig.
2, 3 Covering with mesh graft in a five-year-old girl burned with hot water. |
|
RESUME Pendant la période
1981-1990, 281 patients ont été hospitalis&s dans notre service, 174 rn~les et 107
fernelles. Udge variait entre 2 jours et 14 ans. Dans 72% des cas les brélures étaient
de deuxi&me degré et dans 28% elles étaient de troisi&me degré. Lcs patients
ont ét& divis&s en deux groupes, selon Pdge et la surface brfilée. La méthode
de premier choix &tait la m&thode sans pansement. L'autogreffe a ét&
utilisée dans 76 cas et I'homogreffe, apr&s la détermination de
I'histocompatibilité, dans 4 cas, a cause de la surface brélée &tendue (é0-75%).
On a eu 3 déc~s et le temps moyen d'hospitalisation a ét& 28 jours.
BIBLIOGRAPHY
- Meagher D.P. jr.: Burns, in Swenson's "Pediatric
Surgery", 5tb ed., Appleton and Lange, Norwalk, Connecticut, 1990.
- Caniano D.A., Beaver B.L.: Child abuse. Ann. Surg., 203:
219-224, 1986.
- Munster A.M.: The early management of thermal bums.
Surgery, 87: 29-40, 1980.
- Leicht P., Muchardt 0.: Allografts vs. exposure in the
treatment of scalds - a prospective randomized controlled clinical study. Burns, 15: 1-3,
1989.
- 0' Neil J.A. jr.: Comparison of xenograft and prosthesis
for bum wound care. J. Pediatr. Surg., 8: 705-709, 1973.
- Pietsch J.N., Netscher D.T.: Early excision of major bums
in children: effect on morbidity and mortality. J. Pediatr. Surg., 20: 754-757, 1985.
- Conzales R.V., Heiss W.H.: Twelve years' experience with
the abrasion method for the management of bum wounds in children. J, Pediatr. Surg., 21:
200-201, 1986.
|