| Annals qf the MBC - vol. 5 - n' 1 - March 1992
HISTOPATHOLOGICAL CHANCES IN THE EXPANDED HUMAN SCALP
Hegazy M., Shalby H.A., El-Khalifa M., Ayad H., Ghoraba H.*
Faculty of Medicine, Tanta University, Tanta, Egypt
Plastic and Reconstructive Surgery Unit and Pathology Department
SUMMARY. Histopathological changes of the expanded
human scalp in 10 children aged 2.5 - 12 years old are described. A correlation of the
clinical observations during and after the procedure of expansion with the histological
changes is reported. These changes were found to be present up to six months after removal
of the expanders. Long-term studies, up to two years, are recommended to evaluate the
effect of expansion on the histology and functions of the scalp.
Introduction
Factual histological changes and ultrastructural information describing the
tissue-expansion phenomenon are still scanty in comparison with the rapid increase in
clinical application (Pasyk et al., 1987).
There are sporadic data in the literature connected with the histomorphology of the
expanded skin and soft tissue in the human (Argenta et al., 1985; Pasyk et al., 1987;
Hegazy et al., 1991).
Pasyk et al. (1987) studied the histopathological changes occurring in expanded human skin
at maximum expansion. The expansion process was done at different anatomical sites. There
were two cases of scalp expansion. They used light and electron microscopy in their study.
The stains used were haematoxylin and eosin and toludine blue stains. With light
microscopy, human expanded epidermis showed marked thickening of the stratum spinosum and
flattening of the rete ridges. Human expanded dermis showed marked thinning. Skin
appendages, hair follicles and sweat and sebaceous glands did not show any histological
changes during the process of the expansion.
This study reports a correlation of the histopathological changes and clinical
observations during and after the procedure of scalp expansion in children.
Patients and methods
This study included 10 children presenting to our Unit with post-bum cicatricial
alopecia at various sites of the scalp. The scalp defect was repaired using Dew Coming
Silastic remote valve tissue expanders. One expander and a two-stage procedure were
sufficient in seven cases. In two cases the size of the defect was large and required two
expanders. In the last case the same expander was removed and re-used in the same case
three times to reconstruct an extensive defect on the vertex and sides of the head.
A consent was signed from the parents to take biopsy of normal hair-bearing scalp during
placement of the expander from the expanded scalp during removal and three and six months
later on. The last two biopsies were taken either combined with other procedures or solely
under general anaesthesia.
Every biopsy consisted of 1 x 0.5 cm of skin and subcutaneous tissue down to the
pericranium. The biopsy was fixed in formaline 10% processed in paraffin and stained by
haematoxylin and eosin (H & E), Van Geisson (VG), periodic acid Schifr (PAS), Alcian
blue (AB), Mallory (M) and orcein (0) stains. Examination of these specimens with light
microscopy was carried out.
Results
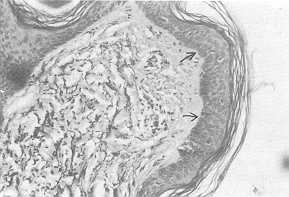
- The epidermis showed focal thickening of the stratum spinosum and flattening of the
rete ridges at maximum expansion (Fig. 1).
These changes were still present 6 months after reconstruction (Fig.
8).
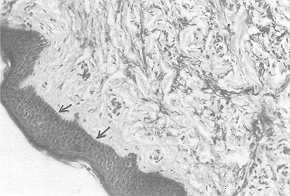
- The dermis showed marked thinning with maximum expansion. The papillary and specially
the reticular dermis were filled with thick bundles of collagen fibres that mostly
oriented parallel to the surface of the skin (Fig. 2).
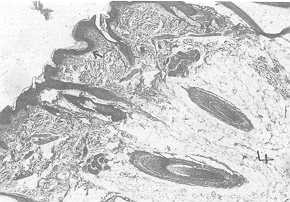
The skin appendages, the sebaceous and sweat glands as well as the hair
follicles did not show any manifest histological changes during maximum expansion.
However, it was noticed that these structures were situated deeper in the deep dermis or
within the subcutaneous fat (Fig. 3).
With maximum expansion there were dilated capillaries in the papillary
derinis, and small blood vessels in the deep dermis were also dilated and filled with
blood. Oedema was noticed in the papillary dermis pushing the elastic fibres away from the
epidermis (Fig. 1). Thinning, shortening and disorientation of the elastic fibres were
also observed (Fig. 1). Three months after expansion the oedema was less manifest and the
elastic fibres became thicker, longer and more oriented and parallel to the skin surface
(Fig. 4).
Acid mucopolysaccharides were found to be increased in the expanded
papillary dermis (Fig. 5, 6) and returned to normal after 6 months. Neutral
mucopolysaccharides were not changed during the expansion procedure.
- The subcutaneous fat subjected to expansion became thinner than normal. The fat cells
became flattened and smaller, and in some parts the fibrous tissue surrounded the fat
cblls or even replaced them. The subcutaneous fat herniated into the reticular or even the
papillary dermis. The skin appendages became present within the subcutaneous fat instead
of being normally in the deep dermis or at the dermo-subcutancous junction (Fig. 3).
- The capsule was found to be formed of four layers:
- the inner layer formed of fibrous tissue and macrophages;
- the second layer: elongated fibroblasts that were pressed within very thick bundles of
collagen oriented parallel to the implant surface;
- the third layer: looser collagen fibres and few blood vessels;
- the outer layer: this is a vascular layer, with dilated blood vessels and more loosely
dispersed collagen fibres and fibroblasts (Fig. 7).
Increased acid mucopolysaccharides were noticed in the fourth layer,
which also contained few elastic fibres (Fig. 7).
All these changes were still present three and six months after expansion (Fig. 8).
Discussion
The histopathological examination of the expanded human epidermis showed focal thickening
and absence of the rete ridges. These changes were still present six months after removal
of the expander. These changes were focal in our study as the specimens were taken from
the periphery of the expanded flaps during removal of the expander. Pasyk et al. (1987)
stated that these changes may be due to a reaction around the expander. The effacement of
the rete ridges may be due to increased pressure of the inflated expander.
Epidermal thickening was reported in guinea-pigs by Austad et al. (1982, 1986), Brobman
and Huber (1985), Johnson et al. (1988) and Vander Kolk et al.
(1988). Austad et al. (1986), reported increased mitotic activity
of expanded guinea-pig skin and they suggested it was due to surgical manipulation or
stretching. Francis and Marks (1977) maintained that skin stretching stimulates epidermal
proliferation only sufficiently to relieve tension or perhaps relieves crowding in the
basal layer which normally inhibits mitosis.
The expanded human dermis, in this study, showed thinning at maximum expansion. It was
filled with thick bundles of collagen fibres. These changes may be due to compression of
collagen fibres as a result of serial expander inflation that decreased the spaces between
the collagen bundles, making them closer and morphologically thickened (Pasyk et al.,
1987). Thinning of the expanded human dermis was reported by Pasyk et al. (1987) and in
the guinea-pig by Cherry et al. (1983). However, Vander Kolk et al. (1988) reported
thickening of guinea-pig dermis with expansion.
In this study, the elastic fibres were found to be thinner, shorter, and more fragmented
and disoriented than normal. These changes improved three months after expansion. The
difference of response between elastic and collagen fibres may be due to the difference in
their nature and structure. The elastic fibres are thin in comparison with collagen
bundles and are wavy (Breathnach et al., 1983). They are therefore the first to be
fragmented and broken with expansion. These are similar to the physiological changes in
elastic fibres with aging, as shown by Lever and Lever (1990). This results in decreased
skin elasticity and may affect the rate of stretching and inflation. It may also play a
role in expander exposure.
The increased acid mucopolysaccharides noticed in our cases that returned to normal six
months after expansion may be due to increased activity of the fibroblasts in the expanded
scalp. Johnson and Helwing (1963) found increased acid mucopolysaccharides in
dermatofibrome and connective tissue around the tumour islands of basal cell carcinoma.
The dilated capillaries in the papillary dermis and small blood vessels in the deep dermis
shown in this study and reported by Cherry et al. (1983) may explain the increased
vascularity of expanded flaps.
Cherry et al. (1983) stated that there may be angiogenesis as a result of stretching and
tissue reaction. These changes may explain the papillary oedema, which may also be due to
compression of the lymphatics by the inflated expander.
The skin appendages did not show any manifest histological changes during the process of
expansion. However, we observed clinically dryness and thinning of the scalp hair during
maximum expansion.
The secretory function of the sebaceous and sweat glands and the hair follicles may be
affected by compression. This may predispose to infection and expander esposure, as we
have previously stated (Hegazy et al., 199 1). Herniation of the subcutaneous fat and the
presence of the skin appendages within this -fat may be a predisposing factor for skin
disruption and exposure of the expander. The function of the skin appendages may also be
affected. Thinning of subcutaneous fat was reported by Pasyk et al. (1987) and its
herniation through the dermis was demonstrated in our study in 199 1.
The four layers of the capsule were previously reported by Pasyk et al. (1988) and the
same was found in this study.
However, the vascularity of the outer layer of the capsule was better clarified in this
study. The presence of elastic fibres in this layer was also evident. The preservation of
the capsule with the advanced or rotated flap is important, especially in extended flaps.
The capsule remnants were present in the specimens examined three and six months after
expansion. Pasyk et al. (1988) reported absence of the capsule two years after expansion
of the cheek in one case. Does the capsule disappear before two years in humans? In the
guinea-pig Pasyk et al. (1988) found that the capsule was absent in the specimens examined
one year after expansion. Does this apply to humans? And is this important clinically?
RÉSUMÉ. Aprés avoir décrit les changements histopathologiques du
cuir chevelu humain expansé, chez 10 enfants ágés de 2,5 jusqu'á 12 ans, les auteurs
distinguent une corrélation entre les observations cliniques pendant et aprés la
procédure d'expansion et les changements histologiques. Ces changements étaient
présents jusqu'á six mois aprés I'enlévement des extenseurs. On recommande d'effectuer
des études á long terme Ousqu'á deux ans) pour évaluer les effects de 1'expansion sur
Phistologie et les fonctions du cuir chevelu.
BIBLIOGRAPHY
- Argenta L.C., Marks M.W., Pasyk K.A.: Advances in tissue expansion. Clin. Plast.
Surg., 12: 159, 1985.
- Austad E.D., Pasyk K.A., McClatchey K.D., Cherry G.W.: Histomorphologic evaluation of
guinea pig skin and soft tissue after controlled tissue expansion. Plast. Reconstr. Surg.,
70: 704-710, 1982.
- Austad E.D., Thomas S.B., Pasyk K.A.: Tissue expansion, divided or loan? Plast.
Reconstr. Surg., 78: 63, 1986.
- Breathnach S.M., Melrose, Bhogal B. et al.: Immunohistochemical studies of amyloid P
component distribution in normal human skin. J. Invest. Dermat., 80: 86-90, 1983.
- Brobmann G.F., Huber J.: Effect of different-shaped tissue expanders on transluminal
pressure oxygen, tension, histopathologic changes and skin expansion in pigs. Plast.
Reconstr. Surg., 76: 731-736, 1985.
- Cherry G.W., Austad E.D., Pasyk K.A., McClatchey K., Rohraich R.J.: Increased survival
and vascularity of random pattern skin flap elevated in controlled expanded skin. Plast.
Reconstr. Surg., 72: 680, 1983.
- Francis A.T., Marks R.: Skin stretching and epidermopoiesis. Br. J. Exp. Path., 58: 35,
1977.
- Hegazy M., Mandour S., Shalaby H.A., Ayad H., Ghoraba H.: The use of tissue expansion
for treatment of alopecia in children. Egypt, J. Plast. Reconstr. Surg., 15: 38, 1991.
- Johnson W.C., Helwing E.B.: Histochemistry of the acid mucopolysaccharides of skin in
normal and in certain pathologic conditions. Am. 1 Clin. Pathol., 40: 123-131, 1963.
- Lever W.F., Lever G.S.: "Histopathology of the skin", I.B. Lippincott Company,
Vol. I (7th ed.), 9-43, Philadelphia, 1990.
- Pasyk K.A., Argenta L.C., Austad E.D.: Histopathology of human expanded tissue. Clin.
Plast. Surg., 14: 435, 1987.
- Pasyk K.A., Argenta L:C., Hassett C.: Quantitative analysis of the thicknessof human
skin and subcutaneous tissue following controlled expansion with a silicone implant.
Plast. Reconstr. Surg., 81: 516-523, 1988.
- Squier C.A.: The stretching of mouse skin in vivo: Effect on epidermal proliferation and
thickness. J. Invest. Dermat., 74: 68-71, 1980.
- Vander Kolk C.A., McCann J.J., Mitchell G.M., O'Brien B.M.: Changes in area and
thickness of expanded and unexpanded axial pattern skin flaps in pigs. Br. J. Plast.
Surg., 41: 284-293, 1988.
|