| Annals of the MBC - vol. 5 - n' I - March 1992
STRUCTURAL ASPECTS IN A BURN UNIT: PROPOSAL OF EXPANDING
MODELS
Magliacani C., Teich Alasia S., Bormioli M., Stella M., Musci
F. *, Holmes J. *
Dept. of Plastic Surgery and Burn Centre, Turin, Italy
* Architects
SUMMARY. This article reviews
criteria for the construction of Bum Centres, with particular regard to the prevention and
control of infection. The functional distribution of space within the hospital building
and the types and characteristics of air-conditioning systems are analysed in detail. It
is pointed out in the conclusion that, apart from structural criteria and surgical and
nutritional treatment, the conscientious respect of hygiene norms is of the highest
importance.
Introduction
The prevention and control of infection in hospital has always represented a major
problem for health services, but for those involved in the care of extensively burned
patients this problem is particularly important.
For this reason during the last fifty years widespread effort has been dedicated to
creating special hospital units in which the probability of infecting the burned surface
could be reduced to a minimum. Centres have been built specifically for the care of
severely burned patients in most countries of the world.
The following topics are analysed in detail:
1. the functional distribution of space within the building;
2. the types and air-conditioning systems.
Both of these factors concern the habitat of the patient, and their
potential for influencing the containment of infection can be manipulated at the levels of
initial design, construction, maintenance and management.
Organization of space for the care of burn patients
In 1972 the Action Committee on Organization of Bum Care, in a report on the distribution
of space within a structure for burn treatment, proposed five different typologies:
1) Individual Care, I patient
2) Bum Service, 2-10 patients
3) Burn Unit, 11-18 patients
4) Bum Centre, 19-26 patients
5) Expanded Burn Centre, 19-26 patients; this included all the supporting structure
necessary for study and research on the subject.
These models represent a sequence of expanding structures each of which
Is equipped to respond to burn treatment requirements in different stituations and in
countries at different stages of development.
While these concepts remain fully valid, we believe it necessary to emphasize certain
basic considerations for the control of infection which influence the distribution of
space.
In order to avoid, as far as possible, the transportation of micro-organisms by carriers
(staff, patients themselves, airborne particles) and prevent their coming into contact
with immunosuppressed patients, priority should be given to two principles:
a) first, reducing the necessity for movement within the unit of staff, patients, waste
material, etc., which implies:
- allocating zones within the ward for each category of patient condition (acute,
non-acute, infected)
- equipping each zone with all the patient-care requirements for daily routine (therapy,
hygiene, staff areas, etc.)
- organizing traffic routes and corridors so that during routine procedures there are no
points of contact between the various zones
- keeping immunosuppressed patients isolated when possible in single rooms;
b) second, inserting pressurized air-locks between rooms with different
asepsis requirements to provide a barrier against airborne micro-organisms.
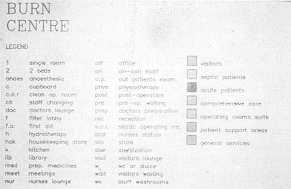
Definition of functional models
Having established these general premises, we will proceed to define the accommodation
necessary for the functioning of burn units of different sizes. For this purpose, with
reference to the first four typologies of the above-mentioned WHO report, a list of
general functions has been drafted which groups together spaces with similar uses or
location requirements. The functions are thus divided into: - patient care (sub-divided
into septic, acute and non-acute) - patient support services - operating suite - visitors'
accommodation.
The specific accommodation necessary for each of the four typologies should then be
established according to function.
Patient bedroom models
A model for a single room for a burn patient (the minimal unit or "Individual
Care") should be a repeatable entity in order to satisfy a wide range of needs while
at the same time allowing standardization of staff routine.
The study for a standard room takes into account the needs of two different kinds of
patient:
a) the patient without particular immunological problems (non-acute)
b) the patient at high immunological risk (acute and septic).
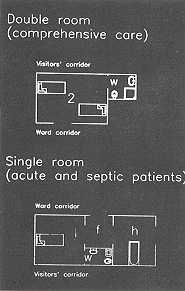
In the first case a room with two beds is proposed, with WC and shower
for each room.
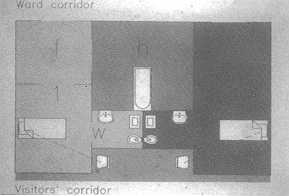
For acute or septic patients a single room is considered essential and, to limit still
further the patient's transfer and the consequent dispersal of organisms, each room should
have an adjoining:
- WC with sluice disposal (separate for each room)
- hydrotherapy tub room (one between two single rooms, accessed through an air-lock from
each side)
- filter/ante-room (separate for each room, positioned between bedroom and access corridor
and acting as air-lock to the tub room) (Fig. 1).
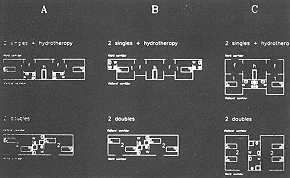
Fig. 2 shows three diagrammatic models (A, B and Q which represent an
evolution of studies for both single and double patient accommodation.
Scheme A is the simplest version to fulfil the requirements of each room type. In scheme B
the different layout creates niches on the outside wall of the single rooms where visitors
may sit and speak to the patients by interphone. In scheme C visitors' bays are provided
both for single and double rooms, and the accommodation is grouped to form a narrower
frontage so that the space occupied by two singles with their ancillary rooms is
equivalent to two doubles. This modularity permits more flexibility in the composition of
layouts for complex ward structure. Version C has therefore been used as the basic room
type for successive development of models for burn care facilities.
 |
 |
| Fig. I |
Fig. 2 |
 |
 |
| Fig. 3 |
Fig. 4 |
 |
 |
| Fig. 5 |
Fig. 6 |
|
Burn care facility models
The main organizational priority in devising models for Individual Care, Bum
Service, Burn Unit and Burn Centre was to eliminate points of contact between sources of
micro-organisms and immunosuppressed patients. To achieve this, which implied the need to
control movement of carriers such as staff, the accommodation was considered in terms of
function groups, and certain key elements were identified:
- separation of patient care areas into self-contained sub-units (septic, acute, non-acute
patients)
- position of operating theatres and services
- position of patient support areas
- position of staff support areas
- separation of visitors' facilities
- separation of connecting corridors between the various zones with air-locks, while
optimizing distances to be covered.
A conceptual layout was derived from these parameters for each of the
four typologies, all having in common:
- a fairly compact general shape in which corridors can be kept to a minimum
- the separation of zones into concentric rings, of which the centre contains support
services and staff areas, the middle band contains the patients' bedrooms, and the other
ring is for visitors.
Individual Care (Fig. 3) is the most simple of the burn care
structures and can receive a maximum of two patients at once. It is intended for insertion
in a hospital ward where all vital support services are available and at the same time
allows considerable autonomy to the burn patient from an asepsis point of view.
Access to the individual care unit should be controlled separately from the rest of the
ward.
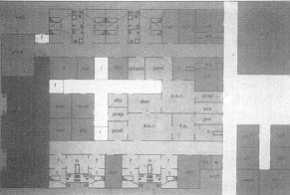
The more articulated typology of the Burn Service (Fig. 4) has a capacity of up to
ten patients in rooms grouped around a central nucleus of support areas. The patient rooms
are divided into sub-groups represented by colours: yellow for septic patients (two beds
in single rooms), red for acute (four beds in single rooms), pink for non-acute (four beds
in double rooms). The support services include:
- operating suite
- nursesI station
- staff changing rooms
- staff lounge
- store
- hydrotherapy tub room.
Each sub-zone has a corridor protected by an air-lock at the entrance.
The visitors' corridor running around the bedroom block is completely separate from
corridors within the ward.
The Burn Service is self-sufficient only to a certain extent and should therefore be
located within or adjacent to general hospital services.
The Burn Unit (Figs. 5, 6) is designed for a full capacity of sixteen patients. The
general layout is again concentric: central nucleus of patient support and general service
area; intermediate band of patient care rooms; external visitors' corridor. The patient
accommodation is represented as follows; yellow for septic patients (four in single
rooms), red for acute (four in single rooms), pink for non-acute (eight in double rooms).
To limit contact between the different sub-zones, each has a separate corridor and a
lounge for staff.
The central block of service areas includes: - a nurses' station
- a kitchenette
- a medication room
- an on-call restroom
- an examination room for out-patients
- staff changing room
- stores
- an operating suite, including a "clean" and a "septic" operating
theatre.
More general accommodation, such as a room for patients' relatives to
consult doctors, is located near the Unit entrance.
The visitors' corridor leads to a visitors' lounge reserved for non-acute patients (access
from the ward is through an air-lock).
Both for general facilities and administration, the Bum Unit would need to be part of a
more complex hospital structure; it has been conceived for the purposes of the model as
occupying all or part of one floor of a building and having three external walls, the
fourth being the access side and the link with the rest of the hospital.
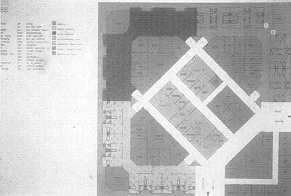
The model of the Burn Centre (Figs. 7, 8) represents a structure which could
receive up to thirty-two patients at once.
 |
 |
| Fig. 7 |
Fig. 8 |
 |
 |
| Fig. 9 |
Fig. 10 |
|
It is subdivided into zones forming concentric bands separated by
corridors and air-locks, and consisting, from the centre outwards, of
- a central nucleus of general service areas
- a zone of patient-support areas for each sub-zone of patient care, located in three
triangular "islands"
- the patient care zone divided into septic, acute and non-acute sub-zones
- the visitors' route around the perimeter.
A series of general service rooms is located close to the entrances of
the building. The central nucleus contains:
- staff changing rooms
- operating suites containing two "clean" and one 41 septic" operating
rooms
- central pharmacy
- sterile store
- central kitchen and store
- on-call restroom
- doctors' lounge.
The position of the central block, angled at 45 degrees, optimizes the
distances to each patient-care zone.
The three triangular "islands", which contain patient-support areas (nursing
station, kitchenette, etc.), allow the staff to remain as much as possible within their
assigned sector, each of which is represented by a colour:
- yellow, for septic patients (8 beds)
- red, for acute patients (8 beds)
- pink, for non-acute patients (16 beds).
Around the perimeter of the bedrooms runs the visitors' corridor (in
green), separate from the ward but leading to a-visitors' lounge accessible only to
non-acute patients.
Nearer to the Burn Centre entrance are the more general service rooms, which do not
require direct contact with the aseptic zones of the patient-care areas.
The schematic model illustrated is conceived as occupying a single floor which would
ideally be at ground level, for reasons of both accessibility and safety, with a basement
level containing technical and auxiliary services, and further plant space and light
sources in the roof. The building could thus be totally independent and could be further
equipped with research laboratories, etc., to constitute an Expanded Burn Centre.
The proposed models are intended to represent a critical tool for the design of burn care
structures with the specific aim of minimizing hospital infection, rather than
architectural solutions adaptable to any real situation.
Air-conditioning in specialist wards
Air-treatment plants are generally required to fulfil two different
orders of requirements: that of guaranteeing certain ideal microclimatic conditions
(temperature, humidity, dilution of smells, etc.) while keeping noise to a minimum, and
that of reaching and maintaining different levels of asepsis in the air, according to the
function of the space. The reduction of bacterial content in the air can be brought about
by either filtration or sterilization. The latter is effected using ultra-violet lamps
positioned either directly in the room or in the air-conditioning ducts as a complement to
the filters.
An air-conditioning plant for operating rooms and for specific areas of specialist wards
(for example acute burn victims) has both an active and a passive function:
a) active: to emit air with a very low microorganism content
b) passive: to impede the passage of air from areas with lower grades
of asepsis to those where the level of sterility is required to be high.
We have selected three systems of high-efficiency cleansing to
illustrate the advancement in the field:
- laminar flow
- directed vertical flow
- Joubert system.
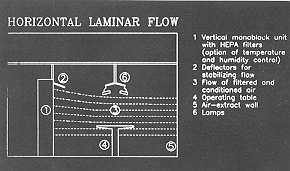
Laminar flow systems (Fig. 9) exist with either horizontal or vertical
orientation. In both cases the air-flow acts on the entire air volume and is characterized
by its very high air-change rate (300-540 volumes/h).
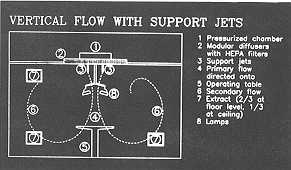
Directed vertical flow (Fig. 10) concentrates its action on the area in which the medical
team is operating and in proximity of the patient.
The system's capacity (20-25 changes/h, which can drop to 15 when rooms are not in use),
although notably lower than that of the laminar flow, is seen to reduce the content of
CY.U. (Colony Forming Units) per cubic metre to a suitable level for delicate operations.
The Joubert system (Fig. 11) is a system based on directed vertical flow for operating
rooms, introducing certain modifications:
- the air
- change rate is of around 50 volumes/h
- of these, 6 vol/h are fresh external air, whi le the other 44 are recycled from the room
and filtered.
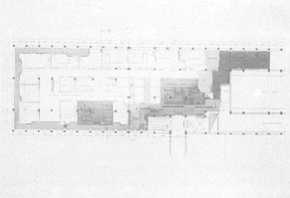
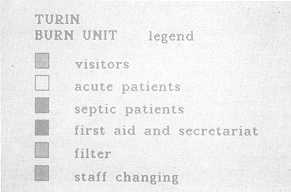
An example of such a structure is the Bum Centre of Turin (Fig. 12),
divided as follows (Fig. 13): - operating suite - patient care, sub-divided into acute and
septic - emergency unit - filter locks - general services.
Conclusion
The provision of increasingly sophisticated treatment by health services and the
incidence, especially in burn cases, of immunosuppressed patients, have, in recent years,
brought about a greater awareness of the problem of hospital infections.
Seen in purely economic terms, the extra costs implied by prolonged hospitalization due to
infection can justify investment in special structures where risks can be reduced to a
minimum.
Therefore the measures illustrated are not solutions in isolation to the problem of
hospital infections. These infections are the result of interacting causes, none of which
should be undervalued or ignored, and should be countered using interacting measures.
For these reasons surgical and nutritional treatment and, above all, the conscientious
respect of hygiene discipline on the part of all members of staff are of fundamental
importance.
RESUME. Les auteurs, après avoir examiné
les critères pour la construction des centres des brdlés, en considérant particulièrement
la prévention et le contréle de l'infection, font une analyse détaillée de la
distribution de Pespace d Fintérieur de I'hépital et des types et des charactéristiques
des systèmes de climatisation. Ils concluent que, d part les critères structuraux et le
traitement chirurgical et nutritionnel, le respect conscientieux des normes hygiéniques
est extrèmement important.
|