Annals of the MBC - vol. 5 - n* 2 -
June 1992
BURN
SCAR CARCINOMA: CASE REPORTS AND REVIEW OF THE LITERATURE
Xie Er-fan, Li A0 (Ngao), Wang
Shi-liang, Kang Shao-yu, Cheng Guang-Xiu
Burn Research Institute, Southwestern
Hospital, Chongqing, Sichuan, People's Republic of China
SUMMARY.
Marjolin's ulcer is defined as a malignant, ulcerating neoplasm occurring in cicatricial
tissue, and is thought to be more aggressive than the other more common varieties of skin
cancers. It has been reported in chronic scars of diverse origins. The following report
describes two cases of burn scar carcinoma. A review is made of the literature pertaining
to the mechanisms, paihological findings, clinical presentation, prognosis, prevention and
treatment of this malignant degeneration of burn scars.
Introduction
The association between thermal burn scars and neoplasia was initially recognized by
Celsus in AD 100 (Treves and Pack, 1930). Jean Nicolas Marjolin, writing in 1828, is
widely credited with the first description of tumour arising in bum scars (Marjolin,
1828). It was De Costa in 1903 who first coined the term "Marjolins's ulcer",
applying it to tumours arising in simple leg ulcers. Although Steffen (1984) and Nancarrow
(1983) have pointed out that Marjolin probably did not recognize the malignant nature of
these ulcers, most other authors have all iden'tified the malignancy found in burn scars
such as Marjolin's ulcer. Today the term "Marjolin's ulcer" is used to describe
malignant turnours arising in many different types of cutaneous scars and chronic wounds,
such as bum scars, chronic venous ulcers, pressure ulcers (decubitus ulcers),
osteomyelitis sinuses, urinary fistulas, pilonidal sinuses, gummata, smallpox vaccination
scars and radiation scars (Abbas and Beecham, 1988; Barr and Menard, 1983; Berkwits et
al., 1986; Fishman and Parker, 1991; Nancarrow, 1983; Steffen, 1984). Butterworths Medical
Dictionary (MacNalty, 1965) now defines Marjolin's ulcer as any cancer arising in
association with a chronic sinus, ulcer or scar.
Case reports
Case 1. A 54-year-old man who incurred secondand third-degree thermal bums in both
lower extremities 40 years previously presented to Southwestern Hospital with chronic
repeated ulceration in the scar area of the right popliteal fossa for 9 years. Treatment
at that time consisted of postage stamp-size skin grafts and healing by secondary
intention. Otherwise, his medical history was not contributory.
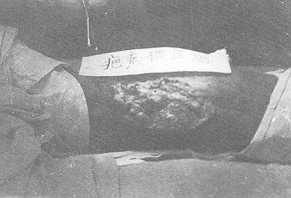
Physical examination revealed the presence of a 10x18 cin umbilicate ulcerated lesion with
verrucose margins and uneven surface on the right popliteal fossa (Fig. 1). The ulcer
exuded a small quantity of purulent, fetid fluid. It was not very painful and easily bled
to the touch. No metastases were detected in either of the inguinal lymph nodes. There was
also scarring affecting most of both lower extremities, with a moderate degree of
hyperplasia and contracture. Incisional biopsy of the ulcer revealed the pathological
diagnosis of squamous cell carcinoma. The patient underwent wide local excision of the
ulcer of the right popliteal fossa and split-thickness skin graft. The wound healed and
the patient was discharged.
Case 2. A 60-year-old man originally sustained a flame burn to the left hand,
without any healing at all, before he was admitted to our hospital after more than 20
years. The bum had been treated without a graft and resulted in significant cicatricial
contractures over the dorsum of the hand as well as the ring and little fingers, with a
chronic recurrent ulcer developing on the dorsum of the hand. The ulcer exacerbated
progressively for 2 months prior to admission and failed to heal on conservative
management. At the time the ulcer measured 8x 10 cm, extending from just proximal to the
wrist joint to the metacarpophalangeal joints. The surface, cauliflower-like and
grey-brown, easily bled to minimal trauma and gave off a foul odour. No axillary or
epitrocheal adenopathy was noted. Biopsies three times revealed "atypical epithelial
proliferation with chronic inflammation" or "squamous pseudoepitheliomatous
hyperplasia". A wide excision of the ulcer on the dorsum of the left hand was
performed with a 2 em margin of grossly normal tissue circumferentially around the ulcer,
followed by the application of a sheet skin graft. Pathological examination of the
surgical specimens under microscope demonstrated that the oncocytes were
characteristically polygonal or oval, and with poor cytoplasm with defined eosin. Circular
or oval nucleoli were very varied in size, and mitoses were usually few in number. The
tumour consisted of irregular masses, cell nests or cord cells and many keratin pearls,
and the intercellular bridges were obvious.
 |
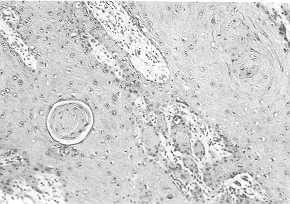 |
Fig.
I Bum scar carcinoma. A view of the large ulcer measuring lOxl8 cm located on the
right popliteal fossa. |
Fig. 2 Burn
scar carcinoma. Microscopic area of invasive tumour having features of well
-differentiated squamous cell carcinoma. Note. karyokinesis, cell bridges and keratin
pearl. (Haematoxylin and eosin x100). |
|
The inflammatory reaction in stroma was
usually very pronounced. microscopic pattern showed no carcinoma cell the border and basal
layer (Fig. 2). The diagnosis was chronic ulcer with malignant change, and
well-differentiated squamous cell carcinoma. The post-operative course of the patient was
smooth and uneventful. He was further administered radiation therapy in the out-patients
department after the wound was healed.
Literature review
Incidence. The incidence of burn scar carcinoma is stated to be "rare".
Although the exact incidence of malignant degeneration of burn scars is not known, 1.2% of
all skin cancer cases (Castillo and Goldsmith, 1968), 2% of squamous cell turnours (Treves
and Pack, 1930; Aarons et al., 1965; Bostwick et al., 1976) and 0.5% of all basal cell
carcinomas (Treves and Pack, 1930) have been reported to originate in burn scars. Sirsat
and Shrikhande (1967) found that up to 6.8% of all squamous turnours originated in burn
scars, and a figure of 25% of malignant transformation in burn scars has been quoted by
them. Nancarrow (1983) indicated that the high incidence in Sirsat and Shrikhande's paper
was probably geographically biased, since in the harsh climates of Asia and the Far East,
body heating devices cause much chronic burning of the skin. The relationship of skin
cancer to prolonged or repeated thermal injury has been demonstrated with the Kangri burn
cancer of India and the Kairo burn cancer of Japan (Treves and Pack, 1930). Both are a
result of the use of hot coals in utensils applied to the abdomen in order to provide
heat. Many users of these devices develop squamous cell carcinoma of the abdominal wall.
The Pi4thogenesis. The precise mechanism of malignant degeneration in burn scars is
not known. Many theories have been proposed. It has been pointed out that every cutaneous
scar subjected to continuous irritation has an increased potential for malignant
degeneration (Glover and Kielm, 1949). Virchow postulated that chronic irritation is a
factor in the initiation of carcinoma, as cited by Treves and Pack (1930), and Horton et
al. (1958). Slow initial healing and scar instability are important in the production of
cicatricial cancers (Treves and Pack, 1,930; Lawrance, 1952). In Lawrance's review (1952)
of cases, 19 showed initial healing of between 3 and 10 years, I I showed no healing at
all before the tumour appeared and I I cases showed episodes of recurrent breakdown.
Nancarrow (1983) reported that 50% of cases exhibited recurrent ulceration of scars or an
origin in a chronic ulcer. Neoplasia is seen with less frequency in burn scars that have
been excised and resurfaced with a graft or flap (Horton et al., 1958; Novick et al.,
1977), giving support to the chronic irritation theory. But even areas which have been
successfully grafted have turned malignant later (Aarons et al., 1965; Sirsat and
Shrikhande, 1967), with both sheet grafts and pinch grafts. This may be related to the
damage of connective tissue. The charred foreign bodies seen by Horton et al. (1958) in
some connective tissue may therefore be of some significance in tumour induction in the
overlying epidermis.
Malignant change may be related to the nature of the scar itself, scars which are greatly
depigmented and thickened being more likely to change (Treves and Pack, 1930; Sirsat and
Shrikhande, 1967). They are less elastic and become ulcerated in response to tension.
Chronic ulceration would therefore appear to be a potent stimulus to neoplasia. Thus, s ,
tress, when applied to any tight or thickened scar situated over joints, is another potent
factor in neoplastic change (Nancarrow, 1983).
Treves and Pack (1930) suggested that decreased vascularity and a weakened epithelium are
unable to withstand the effects of carcinogens, which may be found in the burn wound.
Menkin (1960) studied the role of inflammation and proposed that, in genetically
susceptible persons, exudates produced by endogenous growth-promoting factors can act as
co-carcinogens. Engler et al. (1964) also believed that infection may serve as a
co-carcinogen with scar tissue or "sensitized epithelium". Kennaway (1930) found
that burned human skin produced a tarlike distillate possessing carcinogenic potential.
Safflotti and Shubik (1956) were able to induce skin cancers in 47% of mice whose burned
surfaces were subsequently treated with croton oil. This compared to a rate of only 7% in
burned mice not treated with the oil. Others (Arons et al., 1966; Mackenzie and Rous,
1941) have also postulated that a co-carcinogen is necessary to express the malignant
potential of injured tissue.
Castillo and Goldsmith (1968) proposed that a depressed immunologic state produced by
surrounding scar tissue predisposed to malignant degeneration of the lesion. The absence
of lymphatic drainage from the scar allows a significant delay in host immunologic
recognition, and the antiturnour immunologic response there is poor (Fishman and Parker,
1991). In addition, thermal or other injury may alter cellular deoxyribonucleic acid,
produce mutations, and thus lead to neoplasia (Clairmont et al., 1979).
Pathological types. Squamous cell carcinoma is the most common histologic type of
cancer found. The second most common neoplasm is basal cell carcinoma (Treves and Pack,
1930; Lawrance, 1952). Basal cell carcinoma allegedly occurs,when the burn is more
superficial and the hair follicles and sebaceous glands are intact (Horton et al., 1958).
Carcinomata arising from thermal burn scars are most often of the squamous cell type in
contrast to those arising from radiation bum dermatitis, which are usually of the basal
cell type (Novick, 1977). Other neoplasmas reported to have arisen from burn scars include
melanoma (Lawrance, 1952), osteogenic sarcoma (Drut and Barletta, 1975), firbosarcoma and
adeno-carcinoma (Treves and Pack, 1930), and liposarcoma, carcinoma and carcinoma in
situ (Horton et al., 1958).
Clinical presentation and diagnosis. Burn scar carcinoma occurs at any age and has
no race predilection (Barr and Menard, 1983; Abbas and Beecham, 1988). It occurs more
commonly in males, and the male/female sex incidence has been shown to be 3:1 (Lawrance,
1952; Sirsat and Shrikhande, 1967). It is found predominantly in adults with an average
age of onset of 58 years, range 18 to 84 years (Novick et al., 1977). All cicatricial
cancers have a latent period by definition, during which time an induction mechanism adds
to the initial damage, to produce neoplasia (Nancarrow, 1983). Mean latent periods of 28.5
(Sirsat and Shrikhande, 1967), 32 (Lawrance, 1952) and 32.5 (Treves and Pack, 1930) years
have been quoted with a range of between 8 and 63 years (Treves and Pack, 1930). It has
been reported that the time from the primary burn to the time of onset of the cancer (the
latent period) is inversely proportional to the age of the patient at the time of the burn
injury (Nancarrow, 1983; Lawrance, 1952). The younger the patient at the time of the burn,
the longer the time required for malignant transformation. As the skin ages, it is less
able to withstand trauma. Whether this is due to local mechanisms or the lowering of host
defence mechanisms is not clear (Nancarrow, 1983). In addition, it has been proposed that
the age of the skin and its previous environmental exposure alter its susceptibility to
carcinogenic stimuli (Lawrance, 1952). Acute burn scar carcinoma with a latent period of a
year or less is a rare phenomenon but it has been the subject of many reports in the
literature (Treves and Pack, 1930; Aarons, 1965).
Burn scar cancer occurs in areas of full-thickness or deep non-grafted bums, and it has a
predilection for the extremitites, specifically to flexion creases of the extremites,
where blood supply is decreased and trauma is increased (Aarons et al., 1965; Lawrance,
1952; Novick et al., 1977). This. is in sharp contrast to the distribution of sporadic
squamous cell carcinoma which occurs on the face and neck in more than 90% of cases. Signs
and symptoms associated with the development of the carcinoma include a change in the scar
with formation of a mass or ulcer, possibly with an increase in pain, increasing
discharge, foul odour and bleeding (Ames and Hickey, 1980; Johnson and Kempson, 1965;
Niebauer, 1946; Sedlin and Fleming, 1963). These symptoms may be ascribed to the presence
of infection as opposed to malignancy. Reuler and Cooney (1981) advise increased suspicion
when the margins of the ulcer are verrucous. X-ray films may show bony destruction or
fracture (Johnson, 1965). Bone fixation in cicatricial cancer has been said to be
associated with a poor and Kempson prognosis. The early case report of De Costa (1903)
mentioned this problem, but it must be realized that the cases he dealt with were very
advanced. There is no radiographic evidence of malignancy when the lesion is limited to
the skin (Niebauer, 1946; Sedlin and Fleming, 1963). Biopsy remains the most important
definitive diagnostic procedure, and it should be performed on any suspicious lesion or
any chronic wound, especially those with any recent change in appearance or considerable
drainage (Engler et al., 1964). Niebauer (1946) discourages simple curettage for biopsy
and recommends several sections deep enough to include the subcutaneous tissue. Biopsy
should extract material from multiple sites, including the central areas of the wound as
well as the margins (Lawrance, 1952; Berkwits et al., 1986).
The incidence of metastasis from burn scar carcinoma has varied in different series.
Treves and Pack (1930) reported a 20% incidence, while it was as high as 36% in Aarons'
series (1965) and as low as 15% in Giblin's series (1965). The highest rate of metastasis
was from lower extremity lesions in 54% of cases (Novick et al., 1977). Regional lymph
nodes are overwhelmingly the most frequent sites of metastatic spread (Ames and Hickey,
1980). However, metastases to the brain, liver, lung, kidney, and distant lymph node
basins do occur (Treves and Pack, 1930; Horton et al., 1958; Sedlin and Fleming, 1963).
Reported 3-year mortality rates appear to vary, averaging 34% (Novick et al., 1977).
Mortality at 3 years increases sharply, to 65%, in the presence of involved regional nodes
(Treves and Pack, 1930; Novick et al., 1977; Ames and Hickey, 1980).
Prevention and treatment. The most appropriate treatment for burn scar carcinoma
seems to be prophylaxis. Nancarrow (1983) recommends simple measures such as accident
prevention schemes and avoiding latrogenic provocation by indiscrimintate use of
radiotherapy or noxious chemicals. Once burns or skin trauma have occurred care must be
taken to ensure rapid and good quality early stable healing by skin graft or flap
coverage. Horton et al. (1958) noted that pitted irregular scars trapped debris. This
could produce chronic irritation in a scarred area and this type of scar should therefore
be avoided by good primary treatment and, if present, it should be excised. Once a
full-thickness burn scar is established it should be excised by grafting or tissue
realignment at an optimal time since the incidence of malignant degeneration is quite low
in grafted burn scars. This is particularly true when the burn scar is at flexion creases
and the joints of extremities (Nancarrow, 1983; Novick et al. 1977). In addition, after
initial healing, attention must be paid to those areas of scarring which are unstable or
ulcerated. If ulceration persists for longer than a few months on conservative management,
surgical correction is indicated (Nancarrow, 1983)~ Excision of chronic recurring ulcers
with flap or graft reconstruction is also advocated (Horton et al., 1958).
Treatment of biopsy-proven neoplasia begins with adequate wide local excision with at
least a 2-cm margin, followed by skin coverage (Abbas and Beecham, 1988). Histologic
control of margins is mandatory (Ames and Hickey, 1980). Moreover, the surrounding scar
field may be resected with the tumour excision in the same stage or in subsequent stages
(Nancarrow, 1983; Novick et al., 1977). Amputation is reserved for deep lesions that
extend to bone or joint cavities, as well as for recurrent tumour and possibly for lymph
node metastases (Ames and Hickey, 1980). To avoid obscuring post-operative recurrences by
performing premature reconstructive surgery, skin grafting is the primary modality of
wound closure even though wounds over bony prominences may necessitate later flap
coverage. Novick et al. (1977) have suggested a delay of at least 12 months before one
considers more definitive coverage of the grafted burn wound with a local or distant
pedicle flap.
Pathologic examination revealing atypical pseudoepitheliornatous hyperplasia may pose a
therapeutic dilemma. Johnson and Kempson (1965) reported a case of excision-proven
pseudoepitheliornatous hyperplasia in which malignant regional lymph node metastasis
developed later. These authors believe that all of these cases should be treated as
carcinoma because of the associated difficulties in diagnosis.
The need for regional lymph node dissection is a matter of controversy. Regional lymph
nodes may become enlarged as a result of chronic infection and/or metastases (Engler et
al., 1964; Sedlin and Fleming, 1963), The size of regional nodes is not a dependable
indicator of the presence of malignancy (Berkwits et al., 1986). Some authors (Bostwick et
al., 1976; Novick et al., 1977; Engler et al., 1964) advocate prophylactic regional lymph
node dissection, especially in cases of high-risk tumours such as lower extremity lesions,
in which the incidence of lymph node metastasis has been reported to approach 54% (Novock
et al., 1977). On the other hand, others (Nancarrow, 1983; Barr and Menard, 1983; Abbas
and Beecham, 1988; Aarons et al., 1965; Ames and Hickey, 1980; Horton et al., 1958)
believe that lymph node dissection is indicated primarily in the presence of clinically
positive palpable regional nodes. Bostwick and co-workers (1976) suggested that local
excision of a Marjolin's lesion be followed by elective regional lymph node dissection in
2 to 4 weeks. This recommendation was based on their experience, in which a significant
number of patients experienced aggressive metastases after local excision. It appears
that, given the currently available data, no firm conclusions can be made. At the very
least, local excision with careful follow-up is warranted. In one series (Ames and Hickey,
1980), 98% of all recurrences were seen within 3 years after excision. This included 92%
of all regional lymph node metastases and 88% of the distant metastases.
Little information is available about the efficacy of primary radiation therapy. Ames and
Hickey (1980) used radiation therapy for lesions not suitable for excision or to treat
patients who refused surgical therapy. It has been suggested that postlymphadenectomy
radiation therapy may be appropriate for patients with squamous cell carcinoma of the skin
who experience metastasis to regional nodes (Ames and Hickey, 1980).
The incidence of metastasis after excision of a primary burn scar carcinoma is not
entirely clear. Aarons and colleagues (1966) found that after local treatment 75% of
patients in their series experienced recurrences or metastases leading to death. In the
series of Ames and Hickey (1980), primary treatment of 25 of 41 patients failed, with
approximately one half of these patients exper lencing local recurrences and one half
experiencing metastasis to regional nodes. Berkwits et al. (1986) recommended that
regional nodes should be followed for three years after tumour resection, with monthly
evaluations during the first six months and then bimonthly evaluations.
The prognosis of burn scar carcinoma is poorly documented in the retrospective nature of
these papers, especially because of the lack of full and adequate follow-up (Treves and
Pack, 1930; Aarons et al., 1965; Bostwick et al., 1976; Lawrance, 1952). Prognosis is
primarily related to the local extent of the disease, its anatomical location and the
presence or absence of lymph node metastasis. No single type of scar appeared to carry a
worse prognosis. The survival rates of lesions of the face, neck and upper extremities are
significantly better than those in the lower extremities (Lawrance, 1952; Novick et al.,
1977). Lymph node metastasis is the most important prognostic factor (Treves and Pack,
1930; Novick et al., 1977; Nancarrow, 1983). The patient who survives three years without
metastases has an excellent prognosis (Sedlin and Fleming, 1963).
RÉSUMÉ. L'ulcére de
Marjolin est défini comme un néoplasme malignant et ulcérant du tissu cicatriciel. 11
est consideré plus agressif des autres variétés plus communes des cancers de la peau.
11 peut se manifester dans les cicatrices chroniques de différentes origines. Cet article
décrit deux cas de carcinome observé dans une cicatrice de brúlure. Les auteurs
considérent la littérature pour ce qui concerne les mécanismes, les constatations
pathologiques, la présentation elinique, le pronostic, la prévention et le traitement de
cette dégénérescence malignante des cicatrices de brúlures.
BIBLIOGRAPHY
- Aarons M.S., Lynch J.B., Lewis S.R. et al.: Scar tissue
carcinoma. A clinical study with special references to burn scar carcinoma. Ann. Surg.,
161: 170-188, 1965.
- Abbas J.S., Beecham J.E.: Burn wound carcinoma: case report
and review of the literature. Burns, 14: 222-224, 1988.
- Ames F.C., Hickey R.C.: Squamous cell carcinoma of the skin
of the extremities. Int. Adv. Surg. Oncol., 3: 179-199, 1980.
- Aarons M.S., Rodin A.E., Lynch J.B., Lewis S.R., Blocker
T.G.: Scar tissue carcinoma. Part 11. An experimental study with special reference to burn
scar carcinoma. Ann. Surg., 163: 445-460, 1966.
- Barr L.H., Menard J.W.: Marjolin ulcer: the LSU experience.
Cancer, 52: 173-175, 1983.
- Berkwits L., Yarkony G.M., Lewis V.: Marjolin ulcer
complicating pressure ulcer: case report and literature review. Arch. Phys. Med. Rehabil.,
67: 831-833, 1986.
- Bostwick J., Prendergast W.J., Vasconez L.O.: Marjolin's
ulcer - an immunologically privileged turnour? Plast. Reconstr. Surg., 57: 66-69, 1976.
- Castillo J., Goldsmith H.S.: Burn scar carcinoma. Cancer J.
Clin., 18: 140-142, 1968.
- Castillo J.L., Goldsmith H.S.: Burn scar malignancy in a
possibly depressed immunologic setting. Surg. Foruml 19: 511-513, 1968.
- Clairmont A.A., Hanna D.C., Gaisford J.C., Richardson G.S.:
Marjolin's ulcer. Pa. Med., May: 3 1-33, 1979.
- De Costa J.C.: Carcinomatous changes in an area of chronic,
ulceration, or Marjolin's ulcer. Ann. Surg., 37: 496-502, 1903.
- Drut R., Barletta L.: Osteogenic sarcoma arising in an old
burn car. J. Cutan. Pathol., 2: 302-306, 1975.
- Engler H.S., Fernandez A., Bliven F.E., Moretz W.H.: Cancer
arising in scars of old bums and in chronic osteomyelitis, ulcers, and drainage sites.
Surgery, 55: 654-671, 1964.
- Fishman J.R.A., Parker M.G.: Malignancy and chronic wounds:
Marjolin's ulcer. J. Burn Care Rehabil., 12: 218-223, 1991.
- Giblin T., Pickrell K., Pitts W. et al.: Malignant
degeneration in bum scars: Marjolin's ulcer. Ann. Surg., 163: 29 1-297, 1965.
- Glover D.M., Kiehn C.L.: Marjolin's ulcer: preventable
threat to function and life. Am. J. Surg., 78: 72-780, 1949.
- Horton C.E., Crawford H.H., Love H.G., Leffler R.A.: The
malignant potential of Burn scar. Plast. Reconstr. Surg., 22: 348-353, 1958.
- Johnson L.L., Kempson R.L.: Epidermoid carcinoma in chronic
osteomyelitis: diagnostic problems and management. J. Bone Joint Surg. (AM), 47: 133-145,
1965.
- Kennaway E.L.: Carcinogenic substance and their
fluorescence spectra. Br. Med. L, 1: 1044, 1930.
- Lawrance R.E.A.: Carcinoma arising in burn scars. Surg.
Gynecol. Obstet., 95: 579-588, 1952.
- Mackenzie J_ Rous P.: The experimental disclosure of latent
neoplastic changes in tarred skin. J. Exp. Med., 73: 391-395, 1941.
- McNalty(Ed.): "Butterworths Medical Dictionary".
Butterworths, London, 1965.
- Marjolin J.N.: Ulc~re. In: Adelon N.P. (Ed.):
"Dictionnaire de m6dicine", Vol. 21, 31-50, Bechet, Paris, 1828.
- Menkin V.: Role of inflammation in carcinogenesis. Br. Med.
J., 1: 1586-1594, 1960.
- Nancarrow J.D.: Cicatricial cancer in the south-west of
England: a Regional Plastic Surgery Unit's experience over a 20-year period. Br. J. Surg.,
70: 205-208, 1983.
- Niebauer J.J.: Development of squamous-cell carcinomata
insinus tracts of chronic osteomyelitis. J. Bone Joint Surg. (AM), 28: 280-285, 1946.
- Novick M., Card D.A., Hardy S.B., Spira M.: Bum scar
carcinoma: a review and analysis of 46 cases. J. Trauma, 17: 809-817, 1977.
- Reuler J.13., Cooney T.G.: Pressure sore: pathophysiology
and principles of management. Arm. Intern. Med., 94: 661-666, 1981.
- Safflotti U., Shubik R: The role of burning in
carcinogenesis. Br. J. Cancer, 10: 54-57, 1956.
- Sedlin E.D., Fleming LL.: Epidermoid carcinoma arising in
chronic osteomyelitic foci. J. Bone Joint Surg. (AM), 45: 827-838, 1963.
- Sirsat M.V., Shrikhande S.S.: Histochemical studies on
squamous cell carcinomas of the skin arising in burn scars with special reference to
histogenesis. Indian J. Cancer, 3: 157-169, 1967.
- Steffen C.: Marjolin's ulcer. Am. J. Dermatopathol., 6:
187-193, 1984.
- Treves N,, Pack G.T.: The development of cancer in bum
scars.Surg. Gynecol. Obstet., 51: 749-782, 1930.
|