Annals of the MBC - vol. 5 - n* 2 -
June 1992
RECONSTRUCTIVE
EVALUATIONS ON PLASTIC SURGERY FOR INJURIES AND MASSIVE TISSUE DEFECTS
Belba G., Pepi G.
Clinic of Burns and Plastic Surgery, Hospital N. 2,
Tirana, Albania
SUMMARY. The authors present their
experience in the plastic surgical treatment of massive tissue injuries in the
extremities. After a description of the results of 66 cases, the technical problems of
treatment are discussed. Of special interest is the physiopathological division into three
entities of the avulsed flap. The practical evaluation of flap vascularization creates
premises for a more active surgical attitude, improving the general prognosis.
Introduction
Severe tissue damage usually affects the extremities. This is due to the fact that these
body parts are highly mobile and in continuous activity. The causes of the injury are
various, but the result is often the same: tissue injury, disorder of anatomic regularity,
massive defects combined with bone damage (4, 8). The nature of this shocking trauma
requires the formation of complex teams of specialists, who intervene in their various
sectors (1, 6). Independently of the surgical stabilization of particular anatomic
structures, in the course of the intervention there comes a key moment which decides not
only the success of above procedures but also the life of the extremity. At a certain
point the plastic surgeon "takes the fl6or"; his task is to defend the
reconstructed anatomic formations, to refine the cutaneomuscular system and to secure,
through the covering of injured areas, a normal post-operative period, eliminating sepsis
with its dangerous surprises. Experience has proved that this is the most difficult period
in the treatment of these problematic patients.
In the light of the severe course of the disease and considering the ever wider
manipulations by the plastic surgeon, working in this case as a trauma surgeon, surgical
opinion gradually displaced these patients towards plastic surgery clinics. The grouping
of cases treated during 1990, when the activity of our new bums and plastic surgery
opened, is interesting not only because of the high incidence of this polytrauma, but also
shows the complex methods of treatment.
Material and method of treatment
During 1990, 66 cases of wounds caused by different mechanical traumas were admitted to
our Burns and Plastic Surgery Clinic. This was equivalent to 10.2% of the entire year's
hospitalization. Twelve patients were treated in the intensive care unit. Thirty-one cases
were urgent, while 35 others presented after time periods of up to 1 or 2 months, on the
advice of those who had sent them. The average age of the injured patients was 29 years.
13 were children and 53 adults. 22 were females and 44 males.
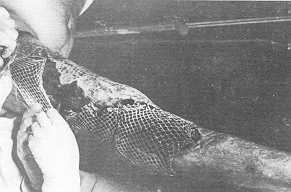
The damage was located in the inferior extremities in 41 cases, while in the other cases
it was in different body regions. The damage also involved some combined regions,
especially femorogluteal and femoroabdominal (Fig. 1, 2).
The patients in reanimation had an average injured tissue surface of about 8.5%, while the
average surface for the patients treated in the wards was 1.6%. Besides subcutaneous
injuries, the fascia and the respective muscle were generally damaged by the causative
agent. In 33 cases (50%) the injury was accompanied by bone fractures, at the level where
the main striking force was applied. Consequently, in addition to the 12 patients treated
in the intensive care unit, 18 others needed elementary reanimating therapy, because of
alterations in the general conditions and as indicated by laboratory analyses.
Before plastic surgery the wounds were explored and debrided. After the orthopaedic or any
other intervention the plastic surgeon retreated the wound, refreshed the cutancomuscular
tissues, setting them as near as possible to their anatomic position. The defect was
permanently covered with skin autografts Of average thickness. In the cases treated
conservatively the wounds were gradually treated and plastic surgery was considered only
after budding of the granular tissue. We adopted this policy because few of the 40 cases
coming from district areas presented in time.
|

|
Fig. I Femorogluteal injury treated with
epidermodermic transplant (mesh graft x 4). |
Fig. 2 Femorogluteal
injury, transplant in the consolidation period (the donor site in the left femoral
region). |
|
In more extensively injured areas, but
also in average or less injured areas, secondary infection developed as a result of
unsuitable and delayed treatment. In laboratory analyses, 8 cases of Proteus mirabilis
were discovered, which further complicate post-traumatic sepsis. Prognosis was complicated
by the coexistence of several micro-organisms. In three cases we observed Proteus and
Staphylococcus aureus, and in two cases Staphylococcus with Bacillus coli. Protection from
sepsis was achieved through the application of powerful antibiotics like gentamicin,
glazidin, amikacin, liquids, electrolytes, tranquillizers, plasma, human albumin,
blood'~tc, as required. The main factor in preventi ' rig sepsis is active surgical
treatment and intensive local care on the basis of the antibiogram.
In the patients treated in the intensive care unit, we performed on average 2.6
interventions, including two epidermodermic plastic operations and usually one debridement
as an intermediate intervention, for the excision of renecrotized tissues.
We performed debridement in only 22.2% of the patients treated in the ward, as a
preparatory intervention before plastic surgery. The average number of interventions in
this group of patients was 1.5, with an average of 1.3 epidermodermic plastic surgery
operations for each case.
Although the damaged surface of the patients treated in reanimation was 5 times as large
as that of the patients treated in the ward, the number of plastic surgery interventions
was slightly greater. This finding shows once again that delayed wound treatment is made
more difficult by the presence of local fibrosis, caused by the deficient initial
treatment.
Results
In 52 (78.79%) of the patients the consolidation of the epidermodermic transplants was
satisfactory. In 6 cases (9.09%), we observed a total autolysis of the transplant, as a
result of infection, with compromising of the general condition in two cases. In these
patients we performed more than two plastic interventions per case. In 8 cases (12.12%) we
were forced to perform a second plastic operation because of the partial autolysis of the
transplant due to different reasons, such as local fibrosis, secretions, and placing of
the transplant in regions contused with fractures or bone fragments.
As a result of severe traumatic injuries, in 15 cases (22.7%) amputations were performed
at different levels of the inferior extremities (4 in the femoral region, one in the leg,
4 in the foot, and 6 in the fingers). A 70-year-old patient treated for a tissue injury
localized in an upper extremity died in the late post-operative period from an acute
attack of myocardia. Out of the 66 patients, 65 achieved wound healing. The average length
of hospital stay for the patients treated in the ward was 34.1 days, and for those in
intensive care 72.1 days.
During hospitalization, in 7 cases various complications were observed such as: pleurisy,
bronchopneumonia, pulmonary thromboembolism, osteomyelitis and local fistula. Treatment
was given as required. Subsequent medical controls will show how many patients suffer from
post-traumatic effects, and how many need reconstructive surgery.
Discussion
A multitude of authors, in anatomic, surgical and laboratory studies, throw light on these
problems, with the aim of treating these wounds in the best way possible, fighting the
causes of infection, reconstructing injured structures, and covering the defects at the
optimal time (3, 4, 5, 9).
Besides the treatment of subcutaneous tissues, aponeurotomy or decompressive fasciotomy
(2, 7) are particularly important. This intervention restores life to the extremity, as it
frees the tissues from oedema, reduces deep haematomas, makes the circulation less heavy,
prevents myoneural deficits from developing and avoids the lodge syndrome.
Our discussion will focus on the treatment of the avulsed flap, a problem which came to
light suddenly while we were studying the interventions carried out in patients treated in
reanimation. Usually, in each case, the interventions were carried out as follows:
- debridement of the wound, followed by skin grafts of the
defects;
- debridement of the renecrotized tissues;
skin grafts of the defects created by
intervention number 2.
As seen from the above list, it is
understandable that the carrying out of a complete necrosis of primarily devitalized
tissues and of those which devitalize (necrotize) later could cut the number of
interventions, reduce the septic condition, and heal the wounds faster. Our opinion is
that this does not happen, firstly, because surgeons wish to leave as much cif the avulsed
flap as possible, as they are convinced that the epidermodermip transplant can in no way
serve as a regional authentic substitute. Secondly, the surgeon is liable to an inevitable
feeling of suspicion regarding the quantity of tissues he must excise in the avulsed flap.
Amid such complexity of feelings this desire inevitably leads to the conviction that more
should be excised. This conviction is however never complete, just as there is no absolute
demarcation limit between the part of flap that will survive and the one that will
necrotize in a second phase. In order to get nearer to this limit and at the same time to
reduce the possibility of error (on either side of the demarcation line), we think it
suitable that the avulsed flap be divided into three physiopathological entities (Fig. 3).
One author rightly considers the avulsed flap an abnormal one (10). Its division into
three specific parts gives us a broader view of the processes going on inside it.
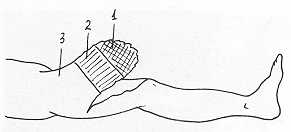 |
Fig. 3 Avulsed
flap in femoral region.
1.necrotic zone 2.ischaernic zone 3.vital zone. |
|
As a result of the direct traumatic
injury, the apex of the flap keeps devitalizing. Thus, the first zone for the excision of
which there is no surgical dilemma is necrotic. At the base of the flap a second zone is
formed, which we would initially call ischaernic, as a consequence of the pulling rather
than of the injurious action of the traumatic agent. Because of this action the vascular
system of the zone undergoes changes, and ecchymotic islands are created in the flap, even
with the formation of thrombi; because of the irregularities of the vessel intima and of
local inflammation, the ischaemic zone becomes fully necrotized. The main pathognomonic
sign of the necrotizing process is the appearance of epidermal blisters. The third zone,
the vital one, is the zone at the base of the flap, on which the pulling action is tense
but not injurious.
The surgeon must be guided by his ability and experience to excise as many tissues as
possible near the demarcation line between the ischaernic zone and the vital zone. This
demarcation line is very difficult to define at first and becomes easily discernible at a
second critical moment. Its existence at the late post-operative period shows that we have
not avoided intervention N' 2, and that we should defend the patient from probable
infection. When technical equipment is perfected and we can define the demarcation line
from the very beginning, new horizons will open up for the microcirculation of the avulsed
flap.
RESUME. Les auteurs pr6sentent
leur exp6rience du traitement, moyermant la chirurgie plastique, des 16sions massives
tissulaires des extr6mit6s. Apr&s avoir d6crit les r6sultats de 66 cas, ils
consi&rent les probl&mes techniques du traitement. La division physiopathologique
du lambeau retranch6 en trois entit&s revet un int6ret particulier. L'&valuation
pratique de la vascularisation du lambeau cr6e la base pour une attitude chirurgicale plus
active, cc qui am6liore le pronostic g6n6ral.
BIBLIOGRAPHY
- Bongard S.F., White H.G., Klein R.S.: Management strategy
of complex extremity injuries. American Journal of Surgery, 158: 151-154, 1989.
- Costecalde M., Gaubert J., Durand J., Barret A., Hormus D.,
Fries F., Trinchero J.F., Chrisment J.N., Demant J.P., Bardier M.: Arrachement subtotal du
membre chez le jeune enfant. Chirurgie p6diatrique, 29: 184-190, 1988.
- Illouz Y.G.: Ludes du tissue graisSeux sous-cutan6. Annales
de chirurgie plastique et &sth6tique, 34: 493-509, 1989.
- Klaner H.L.: Injuries to the extremities: Possibilities for
external fixation. Medical Corps, 1: 34-43, 1986.
- Kirsch J.M., Ventura C., Cambau E.: Population bact6rienne
sur une perte de substance cutane6. Son influence sur la prise des greffes. Annales de
chirurgie plastique et esth6tique, 36: 82-85, 1991.
- Labb6 D., Comp&e J.F., Slama M., Rigot-Jolivet M.:
Traitement en urgence et reconstruction pr6coce des suicid6s de la face par fusil de
chasse. Annales de chirurgie plastique et esth6tique, 33: 140-146, 1988.
- Lagerstrom F.C., Lawrence R., Rowlands J.B., Fischer P.R.:
Early fasciotomy for acute clinically evident posttraumatic compartment syndrome. American
Journal of Surgery, 158: 36-39, 1989.
- Purdue G.G., Hunt L.J.: Multiple trauma and the burn
patient. American Journal of Surgery, 158: 536-539, 1989.
- Seguin P., Aknin J., Van Der Stegen D., Thevenet D.: Les
fascites nécrosantes de la face. Aspects cliniques et th6rapeutiques. Revue de
stomatologie et de chirurgie maxillo-faciale, 91: 374-377, 1990.
- Shindarski B., Gervendov J., Matev J.: Plastiqna hirurgija:
83-85, 1984.
|