Annals o f the MBC - vol. 5 - n' 2 - June 1992
ATRIAL
FIBRILLATION FOLLOWING ELECTRICAL INJURY: A CASE REPORT
Baruchin A.M., * Reisin L., ** Basevich R.
**
* Plastic Surgery Service
** Department of Cardiology, Barrilai Medical Center, Ashkelon, Israel
SUMMARY. A case is reported
of atrial fibrillation following electrical injury in a previously healthy 28-year-old
man. After coming into contact with high-tension electrical current, the patient noted
palpitation and electrical burns of his right upper extremity. An electrocardiographic
diagnosis of atrial fibrillation was made in the emergency department. Although atrial
fibrillation following electrical injury has rarely been reported in the literature, most
cases of severe electrical injury probably warrant cardiac monitoring as a routine
measure.
Electric shock may produce a great variety
of injuries, ranging from a simple unpleasant tingling sensatio n to sudden death. Damage
to muscle and supporting structures is a well-documented pattern of injury. Less is known,
however, about the effects or mechanism of high-tension electrical injuries to the heart.
Ventricular fibrillation and sudden death are a well-known pattern of electrical injury.
In addition various authors have reported ischaemic changes, direct myocardial injury and
myocardial infarction (Chandra, 1990; James, 1990; Kinney, 1982). Atrial fibrillation is
an uncommon complication (Wehrmacher, 1957; Morgan, 1958; Cotoi, 1957). We report a case
of atrial fibrillation occurring immediately after a high-tension electrical injury.
Case report
The patient, a 28-year-old man, was injured at a construction site when he inadvertently
touched a non-insulated 25,000 V A.C. overhead line.
The past history and a review of the systems were noncontributory. There was no history of
any type of cardiorespiratory disease. Physical examination revealed a well-developed,
well-nourished man. He was conscious and had scattered patchlike burns on his right elbow,
right palm and right foot. Sensory and motor examination of all four extremities were
normal. Shortly after admission, the patient complained of palpitation. Vital signs taken
at that time revealed a blood pressure of 150/90, pulse rate of 100 beats/min, totally
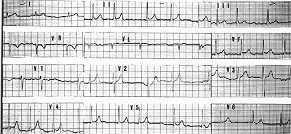
irregular., An electrocardiogram confirmed the diagnosis of atrial fibrillation (Fig. 1).
The patient was given an oral regimen consisting of 0.2 gin of quinidine sulphate every
two hours. Two hours later the pulse was regular, and a normal sinus rhythm was confirmed
by electrocardiogram (Fig. 2).
 |
 |
Fig.
1. Note the absence of P waves with irregular cardiac rhythm. The rate is 70
b/p/min, ventricular axis + SO' with normal configuration of QRS complex. |
Fig.
2. Sinus regular rhythm. The rate is 60 b/p/min, the axis + 60' with normal
configuration of P waves and QRS complex. |
|
Discussion
In our patient, atrial fibrillation was discovered soon after electric shock. Its timely
return to a normal sinus rhythm, its failure to recur, as would be expected in paroxysmal
atrial fibrillation, and its resemblance to other reported cases resulting from electric
convulsive shock therapy or accidental shock indict the electric shock as the cause of
atrial fibrillation in this case. in the present era of attention to cost containment and
bed utilization, providing routine electrocardiographic monitoring of electrically burned
patients for the first 24 hours following injury places a burden on both the patient and
the hospital. The question whether this practice is necessary or merely a luxury based on
remote probabilities was raised by Purdue and Hunt (1986), who summarized their experience
with 58 consecutive patients who sustained high-voltage electrical injuries and concluded
that the routine electrocardiographic monitoring of all these patients during the first 24
hours post-injury was not necessary. The authors felt that monitoring should be
individualized, based on the following criteria:
- history of loss of consciousness or cardiac arrest in the
field;
- documentation of cardiac arrhythmia in the field or in the
emergency room;
- abnormal ECG on admission; l 4. patients whose burn size or
age would require monitoring.
Other patients are either admitted to
nonmonitored beds or discharged from the emergency room, as determined by the size and
site of their injury.
Our case belongs to the second criteria and the lesson learned seems obvious.
RESUME. Les auteurs
décrivent un cas de fibrillation atriale A la suite d'un accident d'origine électrique.
Un homme de 28 ans, précédernment en bonne santé, apr~s avoi r été atteint par
mégard d'un courant de haute tension, souffrait de palpitation et de brfilures
électriques dans 1'extr&mité supérieure droite. Le diagnostic
&Iectrocardiographique de la fibrillation atriale a été effectué dans le services
des urgences. Bien que la fibrillation atriale ~ la suite des accidents d'origine
électrique ait été rarement signalée dans la littérature, le monitorage cardiaque est
justifié dans la plupart des cas de 1ésions électriques graves comme mesure de routine.
BIBLIOGRAPHY
- Chandra N.H., Sin C.O., Munster A.M.: Clinical
predictors of myocardial damage after high-voltage electric injury. Crit. Care Med. 18;
293, 1990.
- Cotoi S., Dragulesco S.I.: Idiopathic persistent
atrial fibrillation precipitated by electrocution in a 40-year-old man. Gior. It. Card.,
4: 80, 1974.
- James T.T., Riddick L., Embry J.H.: Cardiac
abonormalities demonstrated postmortem in four cases of accidental electrocution and their
potential significance relative to hon ' fatal electrical injuries of the heart. Am. Heart
J., 120: 143, 1990,
- Kinney T.J.: Myocardial infarction following
electrical injury. Ann. Emerg. Med., 11: 622, 1982.
- Morgan Z.V., Headley R.N., Alexander E.A. et al.:
Atrial fibrillation and epidural hematoma associated with lightning stroke. N. Engl. J.
Med., 259: 956, 1958.
- Purdue G.F., Hunt J.L.: Electrocardiographic
monitoring after electric injury: Necessity or luxury? J. Trauma, 26: 166, 1986.
- Wehrmacher W.H.: Atrial fibrillation due to
accidental electric shock. JAMA, 165: 349, 1957.
|