Annals of the MBC - vol. 5 - n'2 -
June 1992
INFECTIONS
IN BURN PATIENTS
Reig A., Tejerina C., Codina J., Mirabet V.
Department of Plastic Surgery and Burn Centre,
Hospital La Fe, Valencia, Spain
SUMMARY. An epidemiological
study is made of the infections in the 14é burn patients hospitalized in the Burn Center
of La Fe Hospital (Valencia, Spain) in 1989. 5é (38.4%) patients suffered infection. Mean
patient age was 32.1 years, and é2.5% were males. Mean hospital stay for the infected
patients was 30 days. Mean bum extent was 22.3% TBSA. When burn extent exceeded 20% of the
total surface, the infection rate increased to é5.3%. The association of deep
second-degree and third-degree burns was predominantly related to infection. Electric
current was the commonest aetiology associated with infection in these patients (55.5%).
The burn bed was the most frequent direct cause of infection: alone or in association with
other causes, it accounted for 89.2% of infections. Within the burn bed the most commonly
isolated micro-organism in the first 24 hours was Staphylococcus epidermidis, with Staphylococcus
aureus in the first week and Pseudomona aeruginosa after day 8. Of the 15
hospitalized patients who died in 1989, 9 had suffered infection; in 3% of cases infection
was the cause of death.
Introduction
In spite of considerable advances in the medical and specific treatment of burns,
infection continues to pose the greatest danger to burn patients. In recent years
approximately 73% of all deaths within the first 5 days. post-burn have been directly or
indirectly caused by septic processes (Boswick, 1980).
The aim of the present study was to make an epidemiological evaluation of infection in bum
patients, relating infection to parameters such as burn extent, depth and aetiology,
patient age and sex, and the duration of hospital stay. A study was also made of the
predominant micro-organisms responsible for infection in burns, in the hope of preventing
complications.
The subject of antibiotherapy is being dealt with in ongoing studies.
Patients and methods
An epidemiological study was made of the infections in the 14é burn patients hospitalized
in the Bum Center of La Fe-Hospital (Valencia, Spain) in 1989. During this period, 1825
patients were seen in the hospital, giving an admission percentage of 8% (cf. Tejerina C.
Reig A., Codina J. et al., 1992). Fifty-six (38.4%) patients suffered infection.
Results
Of the 14é burn patients hospitalized in 1989, 5é (38.4%) suffered infection.
Age
The mean age of the patients who suffered infection was 32.1 years (range, 1-84). By age
groups, those aged 21-30 were the most affected (infection in 52.é% of cases), probably
due to the type of lesions involved, followed by those aged 11-20 (25%) (Fig. 1).
Sex
Of the 5é patients with infection, 35 (é2.5%) were males and 21 (37.5%) females. As to
age, infection predominated among males, with the exception of those under age 5 and over
é0, where females prevailed.
Hospital stay
The mean duration of hospital stay was 30 days (range, 3-125).
It should be pointed out that in patients hospitalized for more than 7 days only 10.8%
suffered infection; on the other hand, infection increased to é7.5% among those
hospitalized for over 30 days. Infection clearly contributed to prolonging hospital stay
in some of these cases (Fig. 2).
Mean burn extent was 22.3% TBSA (range, 2-70%). Only 11% of patients had burns affecting
less than 5% TBSA, whereas over 20% was affected in é5.3% of cases. This is also an
important aspect in the prevention and treatment of burn patients (Fig. 3). depth showed
that infection occurred in 20.é% of cases with superficial first- and second-degree
burns, whereas in deep second- and third-degree bums,the incidence increased to 97%. This
reflects the importance of burn depth in septic processes (Fig. 4).
Burn depth
The relationship between infection and burn.
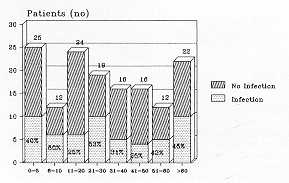 |
Fig. I Age/infection
relationship. Hospital stay (days) |
|
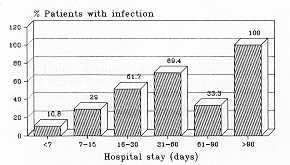 |
Fig. 2 Infection/hospital
stay. |
|
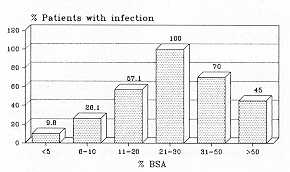 |
Fig. 3 Infection/BSA
relationship, |
|
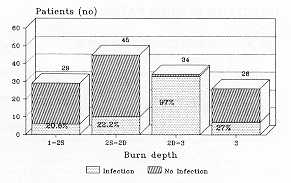 |
Fig. 4 Infection/burn
depth relationship. |
|
Aetiology
Electric current was the aetiology most associated with wound infection in bum patients
(55.5%). Contact burns caused the lowest proportion of infections (0%) (Fig. 5).
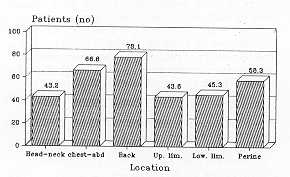
Location
Regarding the location of infection, we limited consideration to the burn bed. The dorsal
region, either isolatedly or in association with other body areas, had the highest
proportion of infections (78.1%); the head and neck were less commonly involved (43.2%).
This clearly reflects the importance of irrigation as an important defence factor against
infections in burns (Fig. 6).
Origin of infection
The bum bed was the origin of infection in most of our patients (89.2%), either isolatedly
or in association with other origins.
Urinary infection, frequently mentioned in other studies, accounted for only 5.3% of our
cases of infection.
The intense contact between patients and nursing stafT in modern burn centres probably
plays a role in this context.
Fig. 7 relates the origin of infection to the successive days of hospitalization. The fact
that the bum bed was an important site of infection during the first 48 hours may be
explained in part by the fact that nearly all these patients had suflered extensive or
deep burns, or else the wounds were caused by electric current; the general conditions of
these were thus so poor that éé.é% of them died.
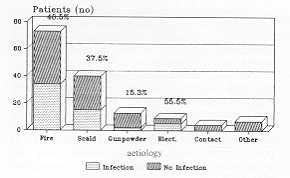 |
Fig. 5
Infection/aetiology relationship. |
|
|
Fig. 6
Location. |
|
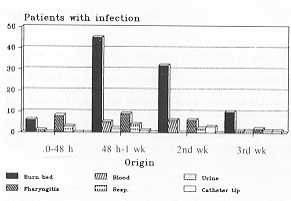 |
Fig. 7 Origin
of infection. |
|
Bacteriology
The most significant results regarding isolated micro-organisms concerned the burn bed (87
cultures performed), blood (44 haemocultures) and catheter tip (23 cultures).
Fig. 8 shows the results of bacterial culture of the bum bed, in relation to successive
days of hospitalization. The most commonly isolated micro-organism was Staphylococcus
epidermidis, with Staphylococcus aureus predominating in the first week and Pseudomonas
aeruginosa after day 8.
Deaths
15 out of the 14é patients died. Of these, 9 (é0%) suffered infection. In 3% of all
cases, infection was the cause of death.
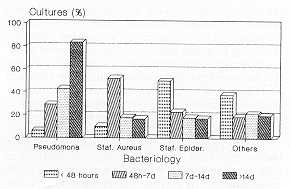 |
Fig. 8 Bacteriology. |
|
Comment
History indicates that the relative importance and the cyclic pathogenicity of various
micro-organisms have changed and may be expected to continue to change as systemic and
topical antibacterial treatment develops (Young, 1977).
Before the discovery of penicillin and the sulphonamides, streptococcal infections were
the most frequent cause of septic death in bums. In the late 1920s and mid-1930s Pack
(192é), Aldrich (1933) and Cruickshank (1935) separately reported that their patients
were colonized with haemolytic streptococci by days 1-é post-burn. However, by the late
1940s Colebrook et al. (1948) noted that streptococcal infections in burns had been
essentially eliminated with the advent of penicillin. As streptococcal infections
declined, Staphylococcus aureus became the major burn pathogen and by the mid-1950s
to early 19é0s was reported by Moncrief and Teplitz (19é4) as the primary isolate
recovered in 75% of the burn patients dying of septicaernia. Once staphylococcal
infections were controlled, the gram-negative organisms came into increasing prominence
and replaced S. Aureus in frequency of occurrence (McMillan, 1982). The decade of
the 1970s heralded an increase in the prominence of yeast, fungi and viruses in the bum
wound flora profile (Foley et al., 1970; Nash et al., 1970; Bruck et al., 1972; McMillan
et al., 1972) with one unit (McMillan 1982) reporting 50-70% of burn patients colonized
with Candida.
Bonny et al. (1984), in their report that spans the period of the late 1970s and early
1980s, indicate that coagulase-positive Staphylococcus has again emerged as the
predominant bum wound pathogenic isolate. In their report yeasts and fungi were recovered
infrequently.
Lowbury (1979) indicates that the more extensive the burn the more likely it is to be
colonized and invaded by micro-organisms. Bonny et al. (1984) demonstrated a significant
association between increasing burn size and increasing incidence of grainnegative
pathogenic organisms. Their report indicates that the incidence of invasive cultures also
increased as burn size increased, with coagulasepositive Staphylococcus the
predominant invasive organism for burns < é0% BSA and Pseudomonas for burns
> 60% BSA.
In the present study we have found that the burn bed is clearly the commonest origin of
infection in burn patients. This agrees with the observations of the above authors,
whereby the risk of infection increases with the percentage of affected total body
surface. We likewise observed an increase in infection incidence with burn depth - with
the exception of those patients who only suffered third-degree bums. In this case the
percentage of infection was lower than in patients with deep second- and third-degree
lesions. However, this observation may be attributed to the fact that in these cases the
percentage of affected body surface was considerably less than in those patients with deep
second- and third-degree burns.
We also found a clear relation between hospital stay and infection risk. The predominant
microorganism depended more on the point within the post-operative period than on the
percentage of affected body surface or other factors: S. epidermidis was the
commonest organism within the first 24 post-operative hours, with S. aureus being
the commonest isolate in the first week and Pseudomonas after day 8.
We agree with other authors (Bonny et al., 1984) in that sepsis caused by Pseudomonas
is a major danger in bums; indeed, they are the most frequent cause of death due to
infection in bum patients.
Within the first 24 hours post-bum the plastic surgeon must be aware of the risk of
infection. In this sense A number of precautions may be stressed:
- measures to combat infection must be reinforced in burn
centres;
- special care must be taken to prevent infections in
patients with deep or extensive burns;
- as hospital stay is prolonged, the risk of infection
clearly increases in bum patients;
- attention should centre on S. aureus, S. epidermidis, and,
particularly, on Pseudomonas;
- bums caused by electric current cause great internal
damage, and are thus especially vulnerable to infection.
RESUME Les auteurs ont effectué une étude
épidémiologique des infections chez les 146 patients hospitalis&s dans le Centre des
Brù1és de I'Hépital La Fe (Valence, Espagne) pendant 1989. 56 (38,4%) patients ont
contracté des infections. Udge moyen des patients était 32,1 ans, et 62,5% étaient
indles. La durée moyenne de I'hospitalisatign des patients infectés était 30 jours. La
superficie moyenne des brillures était 22,3% de la surface corporelle totale. Quand la
superficie de la brfilure dépassait 20% de la surface totale le taux d'infection
augmentait jusqu'A 65,3%. L'association des bralures profondes de deuxiéme et troisiéme
degré était fortement liée A l'infection. Le courant électrique était 1'étiologie la
plus commune chez ces patients (55.3%). Le lit du M11é était la cause directe la plus
fréquente de l'iDfection: seul, on en association avec d'autres causes, il était
responsable de 89,2% des infections. Dans le lit du bré1é les micro -organismes isolés
le plus fréquemment étaient Staphylococcus epidermidis dans les premi~res 24
heures, Staphylococcus aureus dans la premiére semaine et Pseudomonas aerugi .
nosa apres le jour 8. Des 15 patients hospitalisés qui sont morts en 1989, 9 avaient
contracté une infection; en 3% des cas l'infection était la cause du déces.
BIBLIOGRAPHY
- Aldrich R.H.: The role of infection in bums: the theory and
treatment with special reference to gentian violet. N. Engl. J. Med., 208: 299, 1933.
- Bowser-Wallace et al.: Wound flora in children. Burns, 11:
1é, 1984.
- Bruck H.M. et al.: Studies on the occurrence and
significance of yeast and fungi in the burn wound. Ann. Surg., 197: 108, 1972.
- Colebrook L. et al.: The control of infections in burns.
Lancet, 1: 893, 1948.
- Cruickshank R.: The bacterial infections of burns. J.
Pathol. Bact., 31: 37é, 1935.
- Foley F.D. et al.: Herpes virus infection in burn patients.
N. Engl. J. Med., 282: é52, 1970.
- Lowbury E.J.L.: Wits versus genes: the continuing battle
against infection. J. Trauma, 19: 33, 1979.
- McMillan B.G. et al.: Experience with Candida infections
in the burn patient. Arch. Surg., 104: 509, 1972.
- McMillan B.G.: The problem of infections in bums. In Hummel
R.P. (Ed.) "Clinical Burn Therapy", 335, Wright, Bristol, 1982.
- Moncrief J.A., Teplitz C.: Changing concepts in burn
sepsis. J. Trauma, 4: 233, 19é4.
- Nash G. et al.: Candida bum wound invasion. A cause
of systemic candidiasis. Arch. Pathol., 90: 75, 1970.
- Pack J.G.: The pathology of burns. Arch. Pathol. Lab. Med.,
1: 7é7, 192é.
- Tejerina C., Reig A., Codina J. et al.: An epidemiological
study of burn patients hospitalized in Valencia, Spain during 1989. Burns, 18: 15, 1992.
- Young V.M. (Ed.): "Pseudomonas aeruginosa: ecological
aspects and patient colonization", 9, Ist ed., Raven Press, New York, 1977.
|