Annals of the MBC - vol. 5 - n' 2 -
June 1992
HYDROCOLLOID
DRESSINGS IN SMALL AND MEDIUM SPLIT-THICKNESS SKIN GRAFT DONOR SITES?
Santamaria A.B., Oroz J., Pelay M.i.,
Castro J.A., Escudero F.
Plastic and Reconstructive Surgery Unit,
Virgen del Camino Hospital, Pamplona, Navarra, Spain
SUMMARY. There
is currently little agreement among surgeons regarding the dressing of choice for
split-thickness skin graft donor sites. This review examines experience in the treatment
of 30 small and medium graft donor areas with a hydrocolloid dressing (COMFEEL (R)). The
results show important advantages compared to traditional dressings.
Introduction
For centuries wounds have been dressed in order to protect the wound from the harmful
external environment.
The act of covering a wound mimics the function of the epidermis. Haemostasis aided by a
dressing limits blood loss and the dissemination of microbes and toxins, limits oedema,
reduces pain and improves gas and solute exchange between blood and tissue (4).
Although the benefits of covering wounds have been known for years, there was little
progress in dressing development between the 17th century and 1960 (Table 1). Now it is
established that the principal function of a wound dressing is to provide an optimal
healing environment. This thinking began during the 1950s and '60s when research was
published demonstrating that experimentally induced blisters healed more rapidly when the
blister roofs were left intact (9, 11). In 1962, Winter(13) showed that occlusion of
wounds with a polyethylene film in experimental animals resurfaced faster than identical
wounds which were left open to the air. Hinman and Maibach (8) established the beneficial
effect of occlusion on the resurfacing of experimental wounds in normal volunteers. In
these investigations and others, "moist wound healing" was achieved by covering
experimental and non-experimental wounds with an occlusive membrane (3, 10, 12). Between
the '60s and the '80s several adhesive coated polyurethane-film impermeable occlusive
dressings appeared, which were different from oxygenpermeable dressings (1, 2). Another
significant development during the '80s was the introduction of hydrogels and urethane
foam materials. A great deal of progress is expected in the development of dressings
between now and the year 2000.
Semiocclusive and occlusive dressings keep a wound moist and prevent crust formation.
There are different types of moist wound dressings.
The hydrocolloids are direct descendants of materials used historically as ostomy
barriers. A partial list is included in Table 2. In all of them, a water-impermeable
polyurethane outer covering is separated from the wound by hydrophilic colloidal particles
(gum-like materials), such as guar, carboxyineth y Icel lu lose (CMC), gelatin or pectin
formulated in an adhesive mass (usually polyisobutylene). They are opaque and
gasimpermeable.
| 1600 |
1980 |
cotton lint
paper
feathers
dust |
plastic films
hydrocolloids
gums
hydrogels |
| 1960 |
1900 |
non-wovens
plastic films |
non-woven swabs
sleeve dressings
adhesive pads
plaster-strips |
| 1800 |
2000 |
lint fibres
cotton gauze
knitted fibres |
delivery system for
- active agents
- growth factors
- debridement agents
|
|
Table I Wound
dressing evolution |
|
- Duoderm (R)
- J & J Ulcer Dressing (R)
- Comfeel (R)
- Ultec (R)
- Restore (R)
- Intact (R)
- Intrasite (R)
- Hydrapad (R)
Tegasorb (R)
|
|
Table 2 Hydrocolloid
dressings |
|
Patients must be warned of the malodorous
characteristics of the yellow-brown fluid draining under some of these dressings (5).
Although they all provide a moist wound environment for healing, their pliability,
absorbency, dry/wet tack and general appearance may vary.
We present a study carried out on a synthetic occlusive dressing (Comfeel (R) ) in the
treatment of small and medium donor areas.
Material and methods
Comfeel (R) consists of sodium carboxymethyleellulose particles contained in an
elastomer network, forming a pliable plate covered m a semi-permeable polyurethane film
which allows oxygen and water-vapour exchange. It is presented as a square plaque
available in 10, 15 or 20 em sizes.
1. Recent bums |
8
cases |
26.6% |
2. Traumatic
injury |
12
cases |
40
% |
3. Tumoral
excision |
3
cases |
10
% |
4. Venous stasis
ulcers |
5
cases |
16.6% |
5. Diabetic
ulcers |
2
cases |
6.6% |
|
Table 3 Cause
of skin loss |
|
1. Right arm |
4
cases |
13.3% |
2. Left arm |
3
cases |
10
% |
3. Right thigh |
9
cases |
30
% |
4. Left thigh |
12
cases |
40
% |
5. Left gluteus |
1
cases |
3.3
% |
| 6. Right forearm |
1 cases |
3.3 % |
|
Table 4 Location
of donor sites |
|
1. First day |
1
cases |
2. Fourth day |
9
cases |
3. Sixth day |
2
cases |
4. Eighth day |
7
cases |
5. Twentieth day |
1
cases (because of the position
of the donor site for a cross leg flap) |
|
Table 5
Time of first change |
|
 |
 |
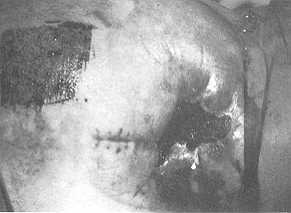
| Fig. I
Donor site that has been just sampled. |
Fig. 2 During
application of the hydrocolloid dressing. |
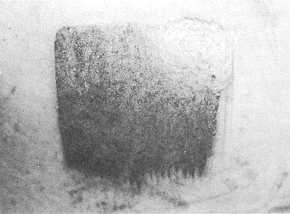 |
Fig. 3 Donor
site healed at day 7. |
|
This synthetic dressing was tested on
small and medium donor sites of 30 patients (23 men and 7 women). The patients' age ranged
from 10 to 88 years (mean age 54). The causes of the loss of skin are shown in Table 3.
The thickness of the split skin graft was from 0.3 to 0.5 ram. Table 4 shows the location
of the donor sites. Once the skin had been sampled (Fig. 1), bleeding was prevented with
compression with saline or H202 gauze for a few minutes. The gauze was then carefully
removed and the site allowed to dry.
The plaque was applied to the area (Fig. 2), taking care to extend it about 2 cm over the
edges of the site to be treated (Fig. 3). In 10 cases the smallest Comfeel (R) plaque was
used, in 9 cases the 15 em size, and in 11 cases the largest size.
Additional compression was achieved with a cr~pe bandage in 23 cases. In 4 other cases,
elastic adhesive tapes maintained mild compression.
The first change of the dressing was performed depending on the conditions of the sampled
zone (Table 5) (Fig. 4, 6).
Application of a fresh plaque was found to be a rapid process. Twelve cases needed a
second fresh plaque and 2 cases a third. The second dressing was applied between day 6 and
day 12. The third change was not necessary before day 8.
Results
The removal of the first plaque and the application of a new one was a rapid process.
Despite their pliability, the wrinkles and air-bubbles during this operation caused some
difficulties. The transparency of the dressing was considered a good property for checking
the healing of donor sites. Moderate pain occurred with the changing of the dressing
during early post-operative care in 5 cases. The dressing was a good option for the
treatment of donor sites in children because the procedure was painless. Three cases of
local contamination occurred, and the normal protocol was suspended. We were not able to
demonstrate infection. One case of allergic reaction was observed (Fig. 5). The average
healing time was 8.15 days, although total epithelialization occurred by day 6 in 4 cases.
The appearance of the site after one month's healing was good, with no hypertrophic or
other pathological scars. There were no differences compared to the fine pink skin of
other forms of treatment of donor site, except for the time that the new cells needed to
cover all the surface. The cost of treatment was reduced compared to that of traditional
dressings.
 |
 |
| Fig, 4 In
some cases, it was necessary to aspirate some exudate without any change of the plaque. |
Fig. 5
One case with folliculitis around the sampled donor site. |
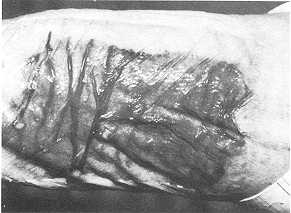 |
Fig. 6 In
one case, it was necessary to keep the plaque for 2 1 days, because the donor site for a
cross leg flap was under a splint. |
|
Discussion
Split-thickness skin grafting (STSC) is a widely used technique for the coverage of
skin defects. It is used by general and plastic surgeons and other surgical specialists
(fo r example, orthopaedics and otolaryngologists). The STSG donor site often has more
problems than the original defect which has been grafted.
An ideal dressing would promote rapid infection-free healing, cause little pain to the
patient. require minimal nursing care and be inexpensive to use.
Although the ideal donor site dressing has yet to be discovered, some individualized
recommendations can be made for specific situations based on current studies.
Small donor sites should be covered with an occlusive or semiocclusive dressing as the
amount of fluid leakage is usually reasonable, and it is cheaper to use. These dressings
are the most comfortable for the patient and allow reepithelialization in approximately 10
days.
Large donor sites can be treated with semi-open dressings (fine mesh gauze). Dressing care
and cost is minimal, and healing occurs predictably in 10 to 14 days.
Conclusions
We demonstrate that Comfeel (R), a hydrocolloid dressing, is a good option, because the
time necessary for the healing of donor sites is shorter and the cost cheaper than for
traditional dressings.
The greatest benefit of occlusive dressings has been to bring about the realization that
the wound and its microenvironment can be greatly modified by whatever covers them. The
dressing is therefore a pharmacological agent, and appropriate modifications may improve
its effect. Occlusive dressing therapy has a bright future, with the purification and
cloning of numerous growth factors. It is likely that we will see "growth
dressings" that combine occlusion with the pulsed delivery of specific growth factors
designed to help a specific clinical problem.
But we must not forget that, in chronic wounds, technical modifications in occlusive
dressings can help to treat the underlying cause. In decubitus ulcers for example, we
could use dressings that redistribute pressure over a larger area.
These are some of the exciting developments that we can expect in the near future with
regard to occlusive therapy.
RESUME 11 n'existe pas aucun
accord général entre les chir-urgiens pour cc qui regarde le pansement de premier choix
dans les sites donneurs de peau A épaisseur variable. Cet article présente les
exp&riences du traitement avec un pansement hydrocolloide (Comfeel (R) ) de 30 sites
donneurs de peau d'extension petite et moyerme. Les résultants montrent des avantages
importants par rapport aux pansements traditionnels.
BIBLIOGRAPHY
- Alvarez O.M., Hofton J.M., Eagistein E.W.: Healing
wounds:occlusion or exposure infection. Infection in Surg., 3: 173-181.
- Alvarez O.H., Mertz P.M., Eaglstein W.H.: The effect of
occlusive dressing on collagen synthesis and epithelialization in superficial wounds. J.
Surg. Res., 35: 142-148, 1983.
- Barnett A., Berkowitz R.L., Mill R. et al.: Comparison of
synthethic adhesive moisture vapor permeable and fine gauze dressings for split-thickness
graft donor site. Am. J. Surg., 145: 379-38 1, 1983.
- Bothwell JW., Rovee D.T.: The effect of dressings on the
repair of cutaneous wounds in humans. In "Surgical Dressings and Wound Healing",
78-97, Harkins K.J. (Ed.), Crosby Lockwood, London,1971.
- Falanga V.: Occlusive wound dressings. Why, when, which?
Arch. Dermatol., 124: 872-877, 1988.
- Fair I., Goldstick T.: Dynamics of water transport in
swelling membranes. J. Cell. Sci., 20: 962-965, 1965.
- Feldman D.L.: Which dressing for split-thickness skin graft
donor sites? Ann. Plast. Surg., 27: 288-291, 1991.
- Hinman C.D., Maibach H.: Effect of air exposure and
occlusion on experimental human skin wounds. Nature, 200: 377-378, 1963.
- Krawezyk W.S.: A pattern of epidermal cell migration during
wound healing. J. Cell. Biol., 49: 247-250, 1971.
- Mandy S.H.: A new primary wound dressing made of
polyethylene oxide gel. J. Dermatol. Surg. Oncol,, 9: 153-155, 1983.
- Odland G.: The fine structure of the interrelationship of
cells in the human epidermis. J. Biochem. Cytol., 4: 529-535, 1958.
- Rovee D.T.: Effect of local wound environment on epidermal
healing. In "Epidermal Wound Healing", Maibach H.L., Rovee D.T. (Eds,), 159-181,
Year Book Medical Publishers Inc., Chicago, 1972.
- Winter G.D.: Formation of scab and the rate of
epithelialization on superficial wounds in the skin of the domestic pig. Nature, 193:
293-294, 1962.
|