Annals of the MBC - vol. 5 - n' 3 -
September 1992
THE
EFFECT OF VERY EARLY ENTERAL TUBE FEEDING ON THE HUMORAL IMMUNITY OF BURNED CHILDREN
Germenis A.E., Achilleos O.A., Stavropoulos-Giokas C.,
loannovich J., Vaos G., Rondras K.
2nd Department of Paediatric Surgery,
Children's Hospital P. & A. Kyriakou & Department of Immunology, General Hospital
of Athens, Athens, Greece
SUMMARY. A comparative study
was made of the effects in severely burned children of very early enteral tube feeding
(VEETF) and of per os feeding. It was found that a) VEETI` produced a
significantly higher elevation of IgG, IgM and C4 serum levels, b) both feeding
schemes caused a significant elevation of C3 scrum levels, that of VEETI` being higher;
and c) neither feeding scheme had a significant effect on lgA scrum levels. It is
concluded that VEETF in severely burned children has a more favourable effect on their
humoral immunity than per os feeding.
Introduction
The term Enteral Tube Feeding (ETF) is used to mean the supply, in liquid form, of all the
necessary nutrient to a certain section of the gastrointestinal tube, through a
nasogastric or a nasointestinal tube, through a gastrostomy or through a jejunostomy. The
term Very Early Enteral Tube Feeding (VEETF), in the case of a burn patient, is used to
mean its performance within the first 6 hours after the accident. Delay in performing ETF
until the motility of the gastrointestinal tube is fully restored may cause a serious
delay in per os feeding. This would increase the frequency of complications, as
well as mortality. VEETF in burn patients contributes to the preservation of the integrity
of the intestinal mucosa and inhibits the translocation of the microbic stems through the
intestinal epithelium to the portal circulation and, consequently, septic complications.
This is the main reason for using it in burn patients.
In 1971, Adibi showed that a short period of deprivation of per os feeding, without
any other nutritive support, causes a quick and extensive decrease of the epithelial cells
of the intestine and a decreased absorption of peptids and aminoacids. In 1974, Levin
proved that ETF is superior to total parenteral feeding, as regards the function and
integrity of the gastrointestinal tube. In experimental models (mice) it has been observed
that under complete feeding suspension the intestinal mucosa becomes atropic within I to 2
days and the weight decreases to half within 6 days. Furthermore, ETF has fewer metabolic
and technical complications.
Feeding
|
Number of children |
Age (years) |
Burn surface (%) |
| VEETF |
15 |
5.4+/-3.7 |
32.6 +/- 14.8 |
| Per os |
6 |
5,2+/-2.5 |
19.5+/- 9.4 |
|
Table I Material |
|
Material and methods
The patients (Table 1) in our study consisted of a group of 15 children (mean age 5.4
years) with an average body surface area burned (BSAB) of 32.6% in whom we performed
VEETF, and a group of 6 children (mean age 5.2 years) with an average BSAB of 19.5% in
whom we performed per os feeding immediately after admission to our Hospital.
As a solution we used the product Reabilan, which contains per litre:
31.5 gr protein (natural oligopeptids)
12.5% energy 39.0 gr lipids (NICT linoleic acid 35.0% energy a-linolenic acid, y-linolenic
acid)
31.5 gr carbohydrate
Osmolality 300 mosmol/It
52.5% energy
There was a continuous performance with an
enteral tube feeding-pump that assured accurate regulation of the application speed. The
parameters valued were the immunoglobulins IgG, IgM, lgA, C3, C4 and PINI. The counting
method was nephelometry. To estimate the changes in concentration of the parameters that
we evaluated, according to the feeding method, in an attempt to avoid the confusing effect
of the nutritional condition and the acute phase reaction - as this is estimated by PINI
values - a multifactor analysis of variance was performed.
This is an inflammation/feeding indicator. Its value depends on the elevation of the acute
phase proteins as well as on the decrease of all the other proteins and especially of
prealburnin, albumin, C3, etc. (Table 2). The acute phase proteins indicate inflammation
and albumin-prealbumin indicates the feeding condition.
PINI values
| 1) Value |
I
minimum risk - no inflammation |
| 2) Values 1-10 |
decreased risk |
| 3) Values 11-20 |
moderate risk |
| 4) Values 21-30 |
high risk |
| 5) Values >30 |
life in danger |
PINI
= |
a
I -acid glycoprotein * CRP |
Albumin
* Prealburnin |
|
Table 2 Prognostic
Inflammatory and Nutritional Index |
|
Results
- VEETF, in contrast to per os feeding, causes
significantly high elevation of the lgC, IgM and C4 serum levels (P= 0.002, 0.015 and 0.03
compared to 0.07, 0.1 and 0.4, respectively).
- The two feeding methods both provide an important increase
of the C3 serum levels (P= 0.000 1 compared to P= 0.0 1).
- The lgA levels do not alter significantly in either of the
two methods.
A small decrease of the IgG value is noted
in the first 48 hours which may be caused by the rapid hydration during these 48 hours.
Between the 3rd and the 10th day, an elevation of the IgG values is noted in both groups
and between the 10th and the 15th day the IgG values increase rapidly in the VEETF group
over the normal limit, in contrast to the per os feeding group, in which the IgG
values remain at the normal lower limit. There is a significantly high elevation in the
VEETF group (Fig. 1). Until the 3rd week, there is a tendency to return to the initial
values and it is supposed that the burned child's organism overcomes the necessity of a
massive immune response in the middle of the 3rd week.
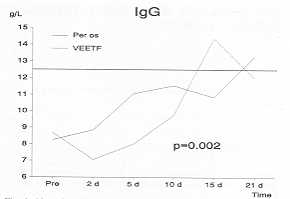 |
Fig. I Alteration
of IgG. |
|
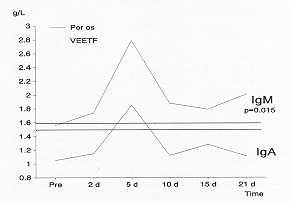
Regarding IgM there is a proportional
alteration (compared to the IgG levels), and a quicker increase of the IgM values is noted
which remain at high levels for a longer time. A significantly high elevation is noted in
the VEETF group (Fig. 2).
A delayed response is noted and the alteration is not of statistical significance. In the
VEETF group the IgA values are however closer to the limits of statistical significance
(Fig. 2).
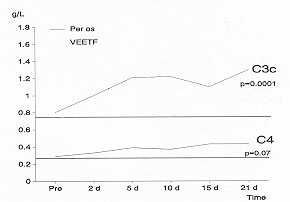
There is an increase of the C3 values between the I Oth and 20th day, which is of
statistical importance. C4 has a higher increase in the VEETF group after the first 4 8
hours, which is also of statistical significance (Fig. 3).
 |
 |
| Fig. 2
Alteration of 19M and IgA. |
Fig. 3 Alteration
of C3c and C4. |
|
Discussion
Per os feeding is sometimes inadequate for the needs of a burn patient, and a face
trauma makes it impossible for technical reasons. Furthermore, the patient's negation
leads to a decreased per os supply. VEETF within the first hours after the
accident, using a nasogastric or nasojejunal tube, is in general the best feeding method
when it can be applied. Modem experimental and clinical studies show that the immediate
application of enteral tube feeding decreases the high metabolic function rate by
decreasing the production of the catabolic hormones (cortisol, catecholamines, glucagon).
It reverses the negative nitrogen balance, more rapidly inhibits intestinal mucosa atrophy
and preserves the intestinal bar.
There is a close relationship between the nutritive condition of a patient and the
function of his immune system. Feeding disorders are considered to be one of the main
factors influencing the process of inflammation. It has been proved that inadequate
feeding alters the immune response. By correcting feeding disorders we restore normal
functioning of the immune system. Inadequate feeding decreases the levels of the
immunoglobulins, the opsonins and the complement.
The complement system, which participates in bacteriolysis, chemotaxis, opsonization and
fixation, is decreased because of inadequate feeding, but immediately increases to normal
limits after restoration of feeding. It has been observed that in patients with feeding
disorders there is an activation of factors that act against the complement system; this
is caused by inadequate feeding of proteins rather than calories. In patients with feeding
disorders complement activity is decreased because of the decrease in cytogenes and
because of the activation of certain factors which induce consumption of complement system
proteins. The IgG, IgM and lgA immunoglobulins are decreased, the rate depending on the
patient's condition. In burn patients serum immunoglobulins are decreased (but this is not
related to the infection or recovery rate). Generally the bibliography is poor regarding
elements that concern the complement, the immunoglobulins and their correlation to enteral
tube feeding, especially VEETF, although it has been performed in burn patients for the
last 4 years. In burned children high and direct caloric support improves survival and the
immune defence and is more successful if associated with VEETF application.
In conclusion, VEETF in children with extensive burn injuries seems to have a more
favourable effect on the main parameters of humoral immunity than per os feeding. VEETF
can supply the calorie requirements of an organism - like that of a burned child - which
needs an alerted immune system capable of becoming fully activated. Our results show that
we succeeded in avoiding disorders of the immune system, which are the main cause of
increased mortality, septicaemia and, in general, non-favourable prognosis.
RÉSUMÉ. Les effets chez les grands
brúlés d'áge pédiatrique de l'alimentation entérale trés précoce par tube (VEETF)
et de l'alimentation per os ont été confrontés. On a trouvé que a) la VEETF
produit une élévation significativement plus haute des niveaux sériques de IgG, IgM et
C4; b) toutes les deux méthodes Walimentation causent une élévation
significative des niveaux sériques de C3 (celle de la VEETF est la plus haute); et c)
aucune des deux méthodes Walimentation ne provoque un effect significatif sur les niveaux
sériques de IgA. On conclut que la VEETF chez les enfanis sévérement brúlés a un
effet plus favorable sur leur immunité humorale que l'alimentation per os.
BIBLIOGRAPHY
- Wilmore D.W., Long J.M., Mason A. et al.: Catecholamines:
Medication of the hypermetabolic responce to thermal injury. Ann. Surg., 180: 653-669.
197,1
- Alexander J.W.: Immunological responses in the burned
patient: NIGMS Burn Consensus report J. Trauma, 19 (suppl.): 887-889, 1979.
- MeArdle A.H., Palmason, Brown R.A., Williams H.B.: Early
enteral feeding of patients with major burns. Prevention of catabolism. Arm. Plast. Surg.,
13: 396, 1984.
- Mochiruliki, Trocki 0., Dominioni L., Brackett K,, Joffe
S., Alexander LW.: Mechanism of prevention of postburn hypermetabolism and catabolism by
early enteral feeding. Arm. Surg., 200: 297-310. 1984.
- loannovich J., Alexakis D., Mantas M., Panayiotou P.,
Tsoutsos D.: The efficacy of early enteral feeding in the treatment of extensive burns.
3rd Meeting of Mediterranean Burns Club, Cairo, 1989.
- Howerton E.E., Kolmen S.N.: The intestinal track as a
portal of entry of Pseudomonas in burned rats. J. Trauma, 12: 835-840, 1972.
- Chithara Y.K., Feirabend T.C.: Endogenous and exogenous
infections with Pseudomonas aeruginosa in burn units. Int. Surg., 66: 237-240,
1981.
- Deitch E.A., Waejima K., Berg R.: Effect of oral
antibiotics and bacterial overgrowth on the translocation of the GI tract microflora in
burned rats. J. Trauma, 25: 385-392, 1985.
- Winchurch R.A., Thurapi J.N., Munster A.M.: Endotoxemia in
burn patients: levels of circulation endotoxins are related to burn size. Surgery, 102:
802-812, 1982.
- MaIjima K., Deitch E., Berg R.: Remotion by bum stress of
the translocation of bacteria from the gastrointestinal tract of mice.Arch. Surg., 119:
166-172, 1984.
- Dudrick S.T.: Nutritional therapy in burned patients. J.
Trauma, 19: 908-909, 1979.
- Bell S.J., Wyatt J.: Nutrition guidelines for burn
patients. J. Am. Diet Assoc., 86: 648-653~ 1986.
- Hildreth M., Carvajal H.F.: Caloric requirements in burned
children: a simple formula to estimate daily requirements. J. Burn Care Rehabil., 3:
78-80, 1982.
- Canningham J.J., Lydon M.K., Russel W.E.: Calorie and
protein provision for recovery from severe burns in infants and young children. Am. J.
Clin. Nutr., 51: 553-557, 1990.
- Pellet P.L.: Food energy requirements. Am. J. Clin. Nutr.,
51: 711-722, 1990.
- Pellet P.L.: Protein requirements in humans. Am. J. Clin.
Nutr., 5 1: 723-737, 1990.
- Dminioni L., Orrawin D., Cheng-Hui F. et al.: Enteral
feeding in burn hypermetabolism: nutritional and metabolic effects of different level of
caloric and protein intake. J. Parent. Enteral Nutr., 9: 269-279, 1985.
- Souba W.W., Bessey P.Q.: Nutritional support of the trauma
patient. Infect. Surg., 3: 727-738, 1984.
- Souba W.W., Schindler B.A., Carvajal H.F.: Nutrition and
Metabolism. In "Bums in Children", 118-144, Year Book Medical Publishers, Inc.,
1988.
|