Annals of the MBC -
vol. 5 - n' 4 - December 1992
MANAGEMENT OF
EYELID BURNS
Maviii E., Kayikcioglu A.
Plastic and Reconstructive Surgery Department, Hacettepe
University, Ankara, Turkey
SUMMARY. Management of eyelid bums
requires great care in the protection of the cornea. A 38-year-old male patient with
severe ectropion was evaluated 8 months after a burn accident and treated by dermabrasion,
overgrafting and cornea transplantation.
Introduction
A large percentage of patients admitted to hospitals with burns involving the face also
have burns of the eyelids (Huang, 1978). Reflex blinking of the eyelids in response to
heat or smoke often protects the cornea and the eyelid margins.
Most eyelid burns are the result of exposure to fire, and not of direct contact with hot
materials or chemicals. If the exposure is brief, a second-degree burn of the eyelid skin
may result. A more intense heat of longer duration may cause a full-thickness burn of the
eyelid skin (Burns, 1979; Converse, 1967; Huang, 1978; Miller, 1979).
Presentation of the patient
A 38-year-old male with second-third degree bums which affected 40% BSA, involving face,
eyelids, neck, arms, hands and chest, was treated at our burns unit for 6 months. The
third-degree burns on the arms, chest and anterior neck were Managed through debridement
and skin grafting. The Opthalmology Department used , non-surgical methods, including
artificial tears and moist,c6vering, in the eyes to prevent drying of the cornea. When the
patient was referred to the Plastic Surgery Department 8 months after the burn injury, he
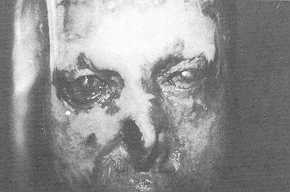
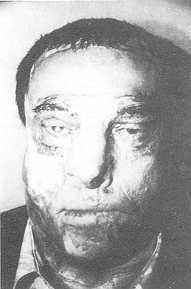
had bilateral ectropion of the lower and upper eyelids. He had nearly complete loss of
vision. His vision was limited to perception of light due to the opacity that had
developed on both corneas. Cornea transplantation was contraindicated because of intensive
vascularization of the sclera and the lack of the protective and lubricating action of the
eyelids (Reim, 1989).
The right half of the nose was absent both in skin and cartilage. The nasal septum was
exposed completely on this side. The left nostril was retracted upwards.
 |
 |
| Fig. Ia. Pre-operative
anterior view |
Fig. lb. Pre-operative
lateral view. |
 |
Fig. lc.
Pre-operative anterolateral view. |
|
 |
Fig. 2.
Intra-operative view of periorbital and nasal reconstruction after completion. |
|
The patient underwent surgery for
reconstruction of the eyelids and nose. In the first operation a forehead flap was used
for nasal reconstruction, the donor site of the flap being covered with a split-thickness
skin graft.
In the second operation the forehead flap was revised. The upper and lower eyelids were
relaxed with horizontal incisions. The burn scars on the periorbital regions were covered
only by a thin layer of epithelium. Unhealthy, fragile epithelium was removed with the use
of a dermabrader. The upper and lower eyelids were then closed tightly with tarsorrhaphy
sutures and the dermabraded periorbital areas were covered with split-thickness skin
grafts. Two strips of hairy skin harvested from the scalp were placed on the defect
created by the upper relaxing incisions for eyebrow reconstruction. After the operation, a
remarkably good protective function of the eyelids was restored and, soon after,
vascularization of the sclera reduced and the oedema subsided.
 |
 |
| Fig. 3a. Late
post-operative period, eyes open. |
Fig. 3b. Late
post-operative period, eyes closed. Successful eyelid function despite a 3 mm closing
defect of the right eyelid. |
|
Two months later, the opacified left
cornea of the patient was replaced with a cornea transplant by the Ophthalmology
Department. The patient is now able to read his newspaper, with a vision of 4/ 10
(according to the Snellen chart) in the left eye. Right eye cornea reconstruction has been
scheduled.
Discussion
The acute management of eyelid burns includes gentle eyelid and eyelash hygiene to prevent
crusting. Topical ophthalmic antibiotic ointments and artificial tears should be applied
frequently. The upper eyelid is responsible for moistening the cornea; when there is a
deep upper eyelid burn the potential for corneal dehydration is therefore present.
Patients with eyelid burns should be examined daily especially while asleep. When the
patient is asleep the voluntary component of lid closure is lost and the cornea may be
partially exposed even if it is completely closed in daytime (McCarthy, 1990). If
nonsurgical measures of corneal protection are not adequate, surgical measures should be
carried out as soon as possible. Although tarsorrhaphy has been advocated for corneal
protection in the past it does not prevent lid retraction in the long term and is not an
appropriate substitute for timely skin grafting (Miller, 1979). If skin grafts are applied
in time there is no reason for corneal ulcers and opacities. Although there are numerous
reports of eyelid burns and corneal transplantation in corneal opacities as separate
entities, there are few descriptions in the literature concerning corneal transplantation
in burned eyelids (Durand, 1990; Reim, 1989; Saparovskii, 1990). If the cornea is
opacified owing to delay in the appropriate treatment, such as in our case, cornea
transplantion cannot be performed unless the inflammatory process in the eye settles down.
This inflammatory process is characterized by ulcerations on the cornea, intense
vascularization of the sclera, and oedema of the conjunctiva (Reim, 1989). The condition
of the eyes develops remarkably after tarsorrhaphy, but if there is tissue lossl as in
deep burns, this procedure should always be followed by grafting. The grafting of the
periorbital region should include not only the obvious defects but also the unhealthy
epithelium -covered areas, to prevent contracting of the tissue in the long-term follow-up
of the patients.
RÉSUMÉ. Le traitement des brúlures de la
paupiére exige des soins trés méticuleux pour protéger la cornée. Les auteurs
décrivent un patient ágé de 38 ans atteint d'ectropion grave qui a été traité, huit
mois aprés 1'incident qui a provoqué la brúlure, moyennant la dermabrasion, la
couverture avee greffe, et la transplantation de la cornée.
BIBLIOGRAPHY
- Brent B.: Restoration of thermally injured facial features.
In "The Artistry of Reconstructive Surgery", 439-445. Mosby, St.Louis, 1987.
- Burns C.L., Chylack L.T. jr.: Thermal burns: the management
of thermal burns to the lids and globes. Ann. Ophthalmol., 11: 1358-1368, 1979.
- Converse J.M.: Burn deformities of the face and neck.
Surgical Clinics of North America, 47: 323-354, 1967.
- Durand L., Fages F.: Inlay corneo-conjunctival lamellar
graft, preliminary step in surgical treatment of the sequelae of corneal burns. J. Fr.
Ophtalmol., 13: 17-23, 1990.
- Engrav L.H., Heimbach D.M.: Excision of burns of face.
Plast. Reconstr. Surg., 77: 744-751, 1986.
- Huang T.T., Blackwell S.J.: Burn injuries of the eyelids.
Clin. Plast. Surg., 5: 571, 1978.
- Press B.: Thermal and electrical injuries. In "Plastic
Surgery", Smith JW., Aston SJ. (Eds.), 675-730. Little Brown and Company, Boston,
1991.
- McCarthy J.G.: "Plastic Surgery", 787-814,
2153-2237. W.B. Saunders, Philadelphia, 1990.
- Miller T.A.: Bums of the face: Burns around the eyes. In
"Burns: a team approach", Artz C.T., Moncrief J.A., Pruitt B.A.A. jr. (Eds.).
W.B. Saunders, Philadelphia, 1979.
- Reim M., Teping C.: Surgical procedures in the treatment of
most severe eye burns. Acta Ophthalmol., Suppl. Copenh., 192: 47-54, 1989.
- Saparovskii S.S., Lebekhov P.I.: The surgical
characteristics of patients with postburn vascularized leukomas. Oftalmol Zh., 5: 257-61,
1990.
- Silverstein P., Peterson H.D.: Treatment of eyelid
deformities due to burns. Plast. Reconstr. Surg., 51: 38-43, 1973.
- Sloan D.F., Huang T.T.: Reconstruction of eyelids and
eyebrows in burned patients. Plast. Reconstr. Surg., 58: 340-346, 1976.
- Wolfe S.A.: Eyelid reconstruction. Clin. Plast. Surg.,
5:525-532, 1978.
|