| Ann. Medit. Burns Club - voL 6 - n. I - March 1993
THE INFLUENCE OF A VARIETY OF PARAMETERS ON THE OUTCOME OF THE
BURN DISEASE IN ELDERLY PATIENTS
D'Arpa N., Napoli B., Masellis M.
Divisione di Chirurgia Plastica e Terapia delle Ustioni,
Ospedole Civico, USL 58, Palermo, Italy
SUMMARY. A number of parameters
(age, percentage burn, time interval between bum and initiation of resuscitatory therapy,
bum phase, previous pathology, type of treatment) are analysed in relation to the outcome
of the bum disease in patients aged 65 years or more. The analysis shows that deaths are
generally due to the reciprocal influence of all the parameters considered.
We consider patient to be elderly if they
are aged 65 years or over, as this is the age at which, in Italy, workers have to cease
their activity and retire (10).
This investigation examines the influence of a variety of parameters (age, percentage
burn, time interval between burn and initiation of treatment, burn phase, previous
pathology, and medical or surgical treatment) on the outcome of the burn disease in
elderly patients.
Our data are taken from a survey of the clinical files of patients admitted to the
Division of Plastic Surgery and Bums Therapy at Palermo Civic Hospital between 1975 and
1992. During this period 257 burned patients aged 65 or over were admitted, of whom 151
were discharged as clinically well (66 males and 85 females) and the remaining 106 (55
males and 51 females) died.
Before proceeding to the analysis, it may be useful to consider the pathologies existing
prior to the bum (Table 1). Although old age is a normal physiological event, it may also
be a predisposing factor in the development of conditions leading to diseases that
influence the outcome of the burn (2).
Analysis of the data
Age
With regard to the effect of age on the outcome of the
burn (Fig. 1), there was a progressive percentage increase in the number of deaths, and a
corresponding decrease in the survival rate, as age increased.
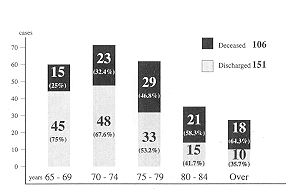 |
Fig. 1 Outcome:
Distribution according to age group |
|
In patients aged over 84 years the. death
rate (64.3%) was nearly double the survival rate (35.7%).
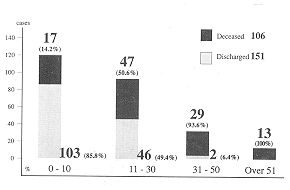
Percentage bum
Considering the patients from the
point of view of burned body surface (Fig. 2), we can see, as in- the case of age, an
increase in the death rate as a function of increased burn extent; the death rate was
93.6% in patients with over 31% burns and 100% when burns exceeded 5 1 %.
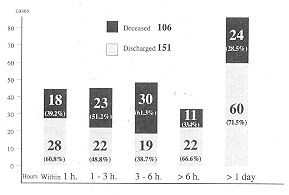
Time interval between burn and hospital admission
Fig. 3 shows the number of deaths and
discharges in relation to the time period between the burn and the beginning of
resuscitatory treatment. As with the age and percentage burn parameters, the increase in
the time period before the patients were admitted corresponded to an increase in the death
rate.
 |
 |
| Fig. 2 Outcome:
Distribution according to % burn |
Fig. 3 outcome:
Distribution according to time interval between burn and hospitalization |
|
The number of discharges exceeded that of
deaths when admission was less than 1 h after the trauma (60.8% and 39.2% respectively,
out of 46 patients); the percentage of discharges was slightly less than that of deaths
when admission was between 1 and 3 h after the trauma (48.8% and 51.2% respectively, out
of 45 patients). The percentage of discharges dropped further when resuscitatory therapy
was initiated between 3 and 6 h after the burn (38.7% and 61.3% respectively, out of 49
patients).
Admission occurring after longer periods shows more survivals than deaths. This apparently
contradictory finding is due to the fact that these patients had been transferred from
other hospitals where they had received early resuscitatory treatment, or else were
patients with deep but not extensive burns.
Burn Phase
Regarding death in relation to the
burn phase (Table 2), 33 patients (31.2%) died during the emergency phase, i.e. within
48-72 h of the burn, 54 patients (50.9%) died in the acute period (i.e. from the 4th day
of hospitalization until surgical therapy), and 19 patients (17.9%) died in the successive
period (chronicization phase). We include in this last group patients who could not be
subjected to the surgical treatment which they in fact required, owing to various severe
complications.
Previous pathology and the burn phase
Table 3 shows the influence of
previous pathology in relation to the burn phase. The pathology was usually not stated in
the case of patients arriving in severe conditions and living alone, and in rare cases was
negative (i.e. the, patients were apparently healthy).
Multiple pathology (diseases involving two or more organs or systems, including without
exception in our cases the cardiovascular system) and isolated cardiovascular pathology
were the conditions most frequently present in elderly patients who died (43.5% and 22.8%
respectively). A comparison between Table 3 and Table 1 shows that death occurred in 50.5%
of patients with multiple pathology and 33.1% of patients with cardiovascular pathology.
Four out of the 11 patients with respiratory pathology died (36.3%), 4 out of 8 with
diabetes (50%), and 4 out of 7 with neuropsychiatric pathology (57.1%).
Type of treatment
Fig. 4 shows the distribution of
patients on the basis of the type of treatment given, in deceased patients and in patients
who recovered. As can, be seen, out of the 151 discharged patients 58.9% were subjected to
surgical therapy and 41.1% received only medical treatment. Among the deceased patients
there was a marked prevalence in the number of nonsurgically treated patients (87.8%) over
medically treated patients (12.2%).
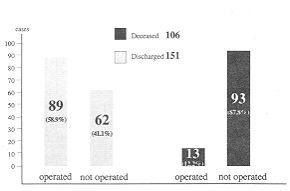 |
Fig. 4 Outcome:
Distribution according to type of treatment |
|
| Type of Pathology |
N* Cases |
% |
| Various |
91 |
35.5 |
| Cardiovascular |
60 |
23.4 |
| Not stated |
59 |
23 |
| Respiratory |
11 |
4.3 |
| Gastroenteric |
9 |
3.6 |
| Diabetes |
8 |
3.1 |
| Neuropsychiatric |
7 |
2.7 |
| Neoplastic |
6 |
2.3 |
| Genitourinary |
3 |
1.1 |
| Osteclarticular |
2 |
0.7 |
| Blood (Anaemia) |
1 |
0.3 |
| Ltotal |
257 |
100 |
|
Tab. 1 Outcome:
Distribution according to previous pathology |
|
Discussion
We have seen that out of the 257
elderly burn patients admitted 106 (41.3%) died and 151 (58.7%) were discharged as
clinically well.
Other reviews of case histories also show a high death rate. Baux et al. (4) reported a
death rate of 59% (22 out of 37 patients) among elderly patients (age 70 years or over)
admitted over a 3-year period (1983-85).
Li Bing-guo et al. (6) reported 36 deaths (32.7%) out of a total of 110 elderly burn
patients (age 65 years or over) admitted over a 10-year period (1978-88).
The above authors stress the important role of age in determining the high mortality rate,
referring to factors such as limited physiological reserves, diminished defence
mechanisms, and previous pathologies. In the elderly these factors significantly impair
the capacity to overcome the shock, infection and metabolic disturbances that frequently
occur in more extensive bums.
| Phase |
Deaths |
% |
| Emergency
phase |
33 |
31,2 |
| Acute phase |
54 |
50.9 |
| Chronicization
phase |
19 |
17.9 |
| Total |
106
|
100 |
|
Tab. 2 Outcome:
Distribution of deaths according to burn phase |
|
| Type of
Pathology |
Deaths |
Total |
| |
Entergency
pluise |
Acute phase |
Chronicintion
phase |
|
| Various |
13 |
25 |
8 |
46
(43.5%) |
| Cardiovascular |
4 |
14 |
3 |
21
(19.9%) |
| Not stated |
11 |
7 |
6 |
24
(22.8%) |
| Respiratory |
1 |
2 |
1 |
4
3.7%) |
| 0a`truenteric |
1 |
- |
- |
10.9%) |
| Diabetes |
1 |
3 |
- |
43.7%) |
| Neuropsychiatric |
1 |
2 |
1 |
43.7%) |
| Neoplastic |
- |
1 |
- |
10.9%) |
| Genitorrinary |
1 |
- |
- |
10.9%) |
| Osteoarlicular |
- |
- |
- |
- |
| Blood (Anaernia) |
- |
- |
- |
- |
| Total |
33 |
54 |
19 |
106
(100%) |
|
Tab. 3 Outcome:
Distribution of deaths according to previous pathology and burn phase |
|
Age, associated with burn extent, is thus
a critical factor. According to our data, and as confirmed by other data in the
literature, the upper limit of the burned surface area for which the elderly burn patient
has some expectation of survival is 30%. Hartford and Ziffren (11) report no cases of
survival in elderly burn patient with burns in more than 30% of body area. In our survey,
only 2 out of 31 patients with burns in 31 to 50% body surface area survived.
| Causes of
death |
N* of Cases |
% |
| Shock and acute renal failure |
23 |
69.7 |
| Respiratory failure |
8 |
24.3 |
| (inhalation damage) |
|
|
| Acute pulmonary oedema |
1 |
3 |
| Myocardial infarction |
1 |
3 |
| Total |
33 |
100 |
|
Tab. 4 Early
mortality. Distribution according to cause of death |
|
It is interesting to note that in both
these cases the patients were aged 65-69 years, had unimportant pathologies (gastritis in
one and arthropathy in the other), were admitted after a delay of no more than 3 hour, and
were subjected to only one surgical operation.
The time interval between the burn and the initiation of therapy is another critical
factor. The burn determines a loss of fluids which makes it necessary to administer other
fluids intravenously in order to reintegrate the loss, prevent shock and maintain organic
functions. The greatest loss of fluids from and in burned tissues is thought to occur in
the first 18-24 hours, with its peak in the first 6-12 hours, starting immediately after
the burn (3, 14). For infusion therapy to be effective, as well as adequate in quantity
and quality, it must be initiated as soon as possible, and in the case of patients
admitted late not actually receiving therapy it is essential to make up for lost time.
Pruitt (14), in relation to resuscitatory fluid therapy in the burn patient, noted on the
one hand the presence in most patients of a physiological reserve and effective
compensatory mechanisms and, on the other, the existence of patients who appear to be
refractory to resuscitation. In this latter category he included patients with massive
burns (70% or more total body surface area), the elderly, and patients in whom
resuscitatory therapy was delayed. If the early initiation of resuscitation is thus
fundamental, it is even more vital in the case of elderly patients, whose response to
resuscitation is very slow.
Our survey shows that delayed resuscitation affected early mortality and determined the
causes of death. Nineteen out of the 33 patients (62.7%) who died in the emergency phase
were adniitted, while receiving no therapy, 3 to 6 hours after the burn.
Table 4 shows the causes of death in the emergency phase. As can be seen, 69.7% of the
deaths were due to shock and acute kidney failure secondary to unsuccessful resuscitatory
treatment, which in most cases was delayed in starting. In addition to late initiation of
resuscitatory therapy, other factors played an important role in early mortality, e.g.
very advanced age and considerable burn extent. The mean age of patients in this group was
78 years and the mean burn extent 50%.
Advanced age, considerable burn extent and delayed resuscitatory therapy were also
associated with a condition of previous disease. This last factor has a decisive role in
non early mortality. Baxter (5) points out that the cardiovascular system is the system
most affected by burns, and that, because of the overwork and the high cardiopathy rate in
the elderly, serious cardiac complications are frequent in these patients.
In fact, we found that out of the 73 patients in our survey who died in the acute or
chronicization phase 43 (59%) died of myocardiac infarction or sudden cardiac
decompensation, while the remaining 30 (41%) died either of acute kidney failure (14
cases, 19.1%), bronchopneumonia (7 cases, 9.6%), severe respiratory failure (4 cases,
5.4), acute anaemia (3 cases, 4.1%) or septicaemia (2 cases, 2.7%).
Finally, as regards treatment, we found that 102 patients (39.6%) were subjected to
surgical therapy. Of these 89 (87.2) were discharged as clinically well and the remaining
13 (12.8%) died.
Early surgery was not generally performed; as these patients are elderly we prefer to
subject them to surgical operation after chemical escharectomy (with antibiotic salicylic
vaseline) so that only one operation should be necessary (12, 13). According to this
protocol, the elderly patient is operated on when second-degree burns have healed and
third-degree zones have good granulation tissue ready for skingrafts. In our survey the
elderly patients subjected to surgery were operated on after an average period of 17.9
days, and the average number of operations per patient was 1.2.
With regard to the patients who died, the average number of days of post-operative
survival was 13.6 (range 1-41).
In 3 cases only (23%) the death of the patients on the first day may be presumed to be
related to the surgical operation. The mean age of the 13 patients who died following
surgery was 77.1 years and the mean burn extent was 22.8%; previous multiple pathology was
present in 7 cases (53.8%) and cardiovascular pathology in 6 cases (46.2).
RESUME. Les auteurs analysent divers
paramètres (l'âge, le pourcentage de la brûlure, le temps passé entre le moment de la
brûlure et le commencement de la thérapie réanimatoire, la phase de la brûlure, la
pathologie préexistante, le type de traitement) en fonction de l'issue de la maladie chez
des patients âgés de 65 ans et de plus. Uanalyse montre que les décès sont
généralement dus à l'influence réciproque de tous les paramètres considérés.
BIBLIOGRAPHY
- Anous M.M., Heimbach D.M.: Causes of death and
predictors in burned patients more than 60 years of age. J. Trauma, 26: 135-139, 1986.
- Baldoni E.: "Uassistenza geriatica: concetti e
tecniche di prevenzione e di recupero". Piccin, Padova, 1986.
- Barisoni D.: "Le ustioni ed il loro
trattamento". Piccin, Padova,1984.
- Baux S., Minoun H. Saade H. et al.: Bums in the
elderly. Burns, 15: 239-240, 1989.
- Baxter C.R.: Problemi e complicazioni nella
rianimazione dello shock da ustione. Clin. Chir. Nord Am., Piccin, Padova, 6: 1464-1475,
1980.
- Bing-Guo Li, Wei-Shia Hsu, Tsi-Siang Shih: Causes of
death in aged burn patients: analysis of 36 cases. Burns, 16: 207-210, 1990.
- Burdge J.J., Katz B., Edwards R. et al.: Surgical
treatment of burns in elderly patients. J. Trauma, 29: 214:216, 1988.
- Clark W.R., Fromm B.S.: Burn mortality. The bulletin
and clinical review of bum injuries, 1: 61-62, 1984.
- Coenen J.M.F.H., Klasen H.J., Savery W.: Successful
homografting in an elderly patient with extensive burns using his identifical twin brother
as skin donor. Burns, 16: 225-226, 1990.
- D'Arpa N., Napoli B., Masellis M.: Epidemiology and
prevention of burns at geriatric age. Ann. Medit. Bums Club, 5: 11-14, 1992.
- Hartford C.E., Ziffren S.S.: Improved survival of
burned aged patients with 0.5 per cent silver nitrate. J. Am. Geriat. Soc., 19: 833, 1971.
- Masellis M., Vitale R., laia A.: Surgical and
chemical necrectomy: two methods for debridement of the burn wound. Riv. Ital. Chir.
Plast., 13: 17-22, 1981.
- Masellis M.: Association of salicylic vaseline with
antiseptics or antibiotics in topical treatment of burns. "Care of the Burn
Wound", 1-6, May, Dogo (Eds), Kanger, Basel, 1985.
- Pruitt B.A. Jr.: Reintegrazione idroelettrolitica
nell'ustionato.Clin. Chir. Nord Am., Piccin, Padova, 6: 1439-1463, 1980.
Slater A.L., Slater H., Goldfarb
W.: Effect of aggressive surgical treatment in older patients with burns. J. Bum Care
Rehabil., 6: 527-530, 1989.
|