| Ann. Medit. Bums Club - voL VI - n. I - March 1993
INTRAVENOUS IMMUNOOLOBULAN IN SEVERELY BURNED
PATIENTS FIVE YEARS OF SUCCESSFUL EXPERIENCE
Oliva R.G., Sica I.
Burn Unit, Juan A. Fernandez Hospital, Cervifio
3356, Buenos Aires, Argentina
SUMMARY. Tlis report is a
retrospective study of the therapeutic benefit of parenteral administration of an
intravenous immunoglobulin (IVIG) preparation for reducing infectious complications in 202
thermally injured patients. All the patients received a complex therapy that included in
67 patients high doses of IVIG. The efficacy of the treatment was evaluated according to
the frequency and localization of the infections, clinical response to anti-infectious
therapy, duration of the infectious process, overall time of hospitalization and mortality
rate. The results demonstrate that patients treated with IVIG in addition to antibiotic
therapy had a significant reduction in mortality due to infections. The patients recovered
faster (50% reduction in hospitalization time) from the thermal injury.
Introduction
Infection remains the most frequent
cause of death in burn patients who survive the initial insult of the thermal injury (1).
Development of infection results from one of two main factors: the presence of a
pathogenic agent with enough virulence to colonize the host, and/or a particular state of
immunodeficiency in the host so that his bacterial saprophyte flora can develop and turn
virulent. In most cases a combination of these two factors is observed (2,3).
In severely burned patients, the first barrier against bacterial entrance, the cutaneous
barrier, is lost or severely affected so that the second barrier, the immune system of the
body, becomes the main defence against infection (4,5,6). Both the humoral and cellular
components of this system participate in the fight. However, it is well known that large
burns are associated with a severe immune dysfunction: tl-ds imimmosuppression affects all
components of the immune system including T-cell, granulocyte and phagocyte function.
Serum immunoglobulin levels are severely depressed in large bum injuries especially during
the first week. For these reasons, there have been some therapeutic attempts to stimulate
the immune system with various immunomodulating agents (7) and nutritional support (8).
Replacement therapy with modified or intact immunoglobulins has also been reported (9,10).
This report is a retrospective study of the therapeutic benefit of parenteral
administration of an intravenous immunoglobulin (IVIG) preparation for reducing infectious
complication in 202 thermally injured patients.
Materials and methods
From a total of 498 patients
hospitalized in our Burn Unit at the Juan A. Fernandez Hospital between January 1987 and
July 1991, 162 clinical histories from patients belonging to Class III and IV of severity
were analysed. We included another 40 patients studied in our first experience, during
1986. This totalizes 202 patients, 16-93 years old, 145 male and 57 female. They were
assisted at variable times after the bum episode, ranging from one hour to 18 days.
All the patients received a complex anti-infectious therapy that included, in 67 patients,
high doses of IVIG. 100 mg/kg/day of Endobulin (Immuno AG) was administered three times a
week until control parameters suggested a change in the patient's class of severity.
The following evaluation criteria were used: nutritional (weight, dosage of albumin and
cholesterol), immunological (dosage of serum immunoglobulins, electrophoretic
proteinogram. and peripheral lymphocyte count), infectological (bacteriological culture
with hyssop and punch with homogeneization of the samples and quantification of the
infection).
The efficacy of the treatment was evaluated according to the frequency and localization of
the infection, clinical response to anti-infectious therapy, duration of the infection
process, overall time of hospitalization and mortality rate.
Results
 |
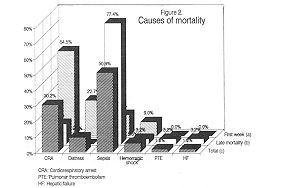 |
Fig. 1 |
Fig. 2 |
|
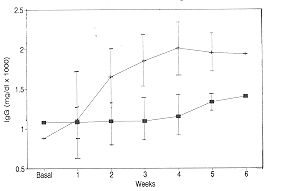
Fig. 1 shows the mean increase of serum IgG in six
patients treated with IVIG as compared with IgG levels of patients treated with
conventional therapy only (control group). The differences found between both groups are
statistically significant.
In the course of the treatment, 53 patients died (26%). The causes of mortality are
recorded in Fig. 2. It was observed that the most frequent cause of death during the first
week of evolution was cardiopulmonary arrest (Fig. 2a), whereas sepsis was the main cause
of mortality in patients who survived the first week of treatment (Fig. 2b). Overall cause
of mortality is shown in Fig. 2c, where it can be seen that sepsis accounts for more than
50% of patient deaths.
The efficacy of IVIG treatment in terms of reduction of mortality in shown in Table 1: 34.
1 % of control patients died as compared to 10.4% of IVIG treated patients. This reduction
is very significant (p < 0.001).
Patients |
N. of
cases |
N. of
deaths |
% |
|
| Control |
135 |
46
|
34.1 |
|
| Treated |
67 |
7 |
10.4
|
p < 0.001 |
|
| Table 1 Global mortality |
|
Patient distribution according to group'of
severity gave similar good results. Table II illustrates the effect of IVIG treatment on
sepsis mortality in patients from Class 111 and IY Most of the deaths occurred in Class
IV: 32.2% were from control patients as compared to 4.76% from the treated patients.
Patients |
Class III |
Class IV |
|
N. of |
N. of |
N. of |
|
N. of |
N. of |
|
|
cases |
cases |
deaths |
% |
cases |
deaths |
% |
|
Control |
1.31 |
76 |
1 |
59 |
19 |
32.2 |
|
Treated |
0 |
25 |
0 |
42 |
2 |
4.76 |
P < 0.001 |
|
| Table II Sepsis mortality |
|
| Patients |
Class III days |
Class IV days |
Total days |
|
| Control |
46.2 |
73.4 |
59.8 |
|
| Treated |
23.2 |
42.9 |
33.1 |
p < 0.01 |
|
| Table III Mean time of hospitalization |
|
The efficacy of the treatment is also
reflected in a significant reduction of hospitalization time (Table 111); treated patients
from Class III stayed 50% less time in hospital than control patients, and patients from
Class IV receiving IVIG benefited with a 32% reduction in hospitalization time.
Discussion
In severely burned patients scrum
immunoglobulins are depressed owing to an increased rate of disappearance, especially of
IgG (11). This may be due to several factors, including increased catabolism, given the
hypermetabolic state of the burn patient and the loss of serum immunoglobulins by wound
exudates.
This condition, together with the loss of the skin barrier, makes the burn patient very
susceptible to infections. In fact, this remain the most frequent cause of death among
these patients (1).
The clinical use of immunoglobulins started in the 1950s, after the Second World War.
These products were for intramuscular use and were indicated in the prevention of viral
infections. Later this was extended to patients with severe immunodeficiencies (12). The
introduction in the 1970s of immunoglobulins for intravenous use allowed their
administration in higher doses. The first preparations were elaborated with methods that
included proteolytic enzymes that degraded the molecule to avoid side-reactions,
frequently observed in previous preparations (13); later on, methods that maintain the
integrity of the molecule were developed but they were chemically modified (14). The most
recent advances are products that contain intact and unchanged molecules of immunoglobulin
that preserve all the properd biological functions of native proteins (15). They are the
so-called third-generation immunoglobulins.
Replacement therapy in burn patients with intact or modified IVIG containing a wide
spectrum of antibodies against a variety of common pathogens resulted in elevation of
serum immunoglobulins (9,10). However, no success was obtained in terms of reduction of
infections and/or mqrtality rate (10).
In this report we present data comparing the efficacy of a complementary IVIG treatment
(third-generation immunoglobulin) to conventional therapy in severely burned patients.
We were able to demonstrate that patients treated with IVIG in addition to antibiotic
therapy had a significant reduction in mortality due to infections (Table 11). We
interpret that this was due to a faster recovery of the patients (50% reduction in
hospitalization time) that enabled us to "rescue" some patients from exposure to
pathogens.
We believe that, in addition to proper hydration of the patient, early escharectomy and
grafting, and specific antibiotic therapy, the administration of intravenous
immunoglobulin is an invaluable tool in the management of bum patients.
RESUME. Cet article est une
étude rétrospective sur les avantages thérapeutiques de l'administration parentérale
d'une préparation intraveineuse d'immunoglobuline (IVIG) pour réduire les complications
infectieuses chez 202 patient brûlés. Tous les patients ont re~u une thérapie complexe
qui incluait, pour 67 patients, des doses élevées d'IVIG. Uefficacité du traitement a
été évalué selon la fréquence et le site des infections, la réaction clinique à la
thérapie anti-infectieuse, la durée du procès infectieux, la période complessive de
l'hospitalisation et le taux de mortalité. Les résultats montrent que les patients
traités avec IVIG en plus de la thérapie antibiotique ont présenté une réduction
significative de la mortalité due aux infections. En outre, les patients ont guéri plus
rapidement des lésions causées par la brûlure (réduction de 50% dans la période de
l'hospitalisation).
BIBLIOGRAPHY
- Sevitt S.: A review of the complications of burns,
their origin and importance for illness and death. J. Trauma, 19: 385, 1979.
- Alexander J.W., Meakins J.L.: A physiological basis
for the development of opportunistic infections. Ann. Surg., 176: 273, 1972.
- Pruitt B. et al.: Opportunistic infections in
severely burned patients. Am. J. Med., March: 146, 1984.
- Kohn J., Cort D.F.: Immunoglobulins in burned
patients. Lancet, 1: 836, 1969.
- Munster A., Eurenius K. et al.: Cell mediated
immunity after thermal injury. Ann. Surg., 177: 13, 1973.
- Munster A.: Immunologic response of trauma and bums.
Am. J. Med., March: 142, 1984.
- Wayinack J.P., Jenkins M. et al.: A prospective
study of thymopentin in severely burned patients. Gynecol. Obstet., 164: 432, 1987.
- Alexander JW: Nutrition and infection: new
perspectives for an old problem. Arch. Surg., 121: 966, 1986.
- Shirani K.Z., Vaughan G. et al.: Replacement therapy
with modified immunoglobulin G in burn patients: preliminary kinetic studies. Am. J. Med.,
March, Suppl. 3A, 76: 175, 1984.
- Waymack J.P., Jenkins M. et al.: A prospective trial
of prophylactic intravenous immune globulin for the prevention of infections in severely
burned patients. Burns, 15: 71, 1989.
- Arturson G., Mogman C.F. et al.: Changes in
immunoglobulin levels in severely burned patients. Lancet, 1: 836, 1969.
- Janeway C.A., Rosen F.S.: The gammaglobulins. IV.
Therapeutic uses of gaminaglobulin. N. Eng. J. Med., 275: 826, 1966.
- Sgouris LT: The preparation of plasmin treated
immune scrum globulin for intravenous use. Vox Sang., 32: 175, 1967.
- Stephan W.: Beseitigung der Komplemententlixierung
von Gammaglobulin dutch chemische Modifizierung mit B-propionolacton. Klin. Chem. u Klin.
Biochimie, 7: 282, 1969.
- Eibl M. et al.: Safety and efficacy of monomeric,
functionally intact intravenous IgG preparation in patients with primary immunodeficiency
syndrome. Clin. Immunol. Immunopath., 31: 151, 1984.
|