| Ann. Medit. Burns Club - vol. 6 - n. 1 - March 1993
GASTROINTESTINAL AND RENAL COMPLICATIONS IN BURN PATIENTS Haberal M., Ozdemir A., Bayraktar U, Oner Z, Bilgin N. Turkish Transplantation and Burn Foundation, Ankara, Turkey SUMMARY. In a period of eleven years, from January 1 1979 to December 31 1989, 915 burn injury patients were admitted to our centre. The ParklaDd formula was used for fluid resuscitation in all patients. In 24 (2.6%) patients gastrointestinal (GI) complications were encountered, 22 with upper GI complications. In 4 patients with massively bleeding ulcer, vagotomy + pyloroplasty or vagotomy + gastrojejunost6my was performed together with suturing of the ulcer. Of the 22 patients with upper GI bleeding, 18 died. The causes of death were massive bleeding in four patients, and septic complications in the others. 19 (2%) of the 915 burn patients required dialysis treatment because of acute renal failure. The reasons for acute tubular necrosis were either multiple organ failure or sepsis. The mortality rate in acute renal failure patients requiring dialysis was 78.9% (100% in flame bum patients and 60% in electrical burn patients). Despite the various sophisticated methods of treatment used in the field of burn injury, gastrointestinal and renal complications still comprise the major problems causing significant morbidity and mortality. Gastrointestinal changes following thermal injury are common and often become manifested by early coffeeground vomiting in major burn cases. The pathogenesis of these lesions and the functional alterations have not yet been clarified (1,2). The renal response to thermal injury is difficult to interpret, but it is quite clear that acute renal failure rarely occurs in cases where prompt and adequate resuscitation is accomplished (1,3). Material and Method In a period of eleven years, from January 1 1979 to December 31 1989, 915 burn injury patients with various types of burns were admitted to our centre. The modified Parkland formula was applied in all patients for fluid resuscitation. In accordance with this formula, 2-3 ml/kg/BSA of lactated Ringer's solution was administered during the first 24 hours. 7he amount of fluid administered varied according to the time of admission of the patients.Urine output was carefully monitored in the first 24 h, considering adequate a urinary output of 0.5 to 1.0 ml/kg body weight/li. In cases of oliguria, sodium bicarbonate, mannitol (20-40 g) and furosemide (40-100 ing) were administered. Persistent oliguria, with acidosis and rising potassium, BUN and creatinine, was treated with peritonea] dialysis or haemodialysis. A double-lumen subclavian catheter (Gambro SCK-102, 20 cm) was used for haemodialysis and/or parenteral alimentation. A urinary catheter and a central venous line were used only in severe cases or as was deemed necessary. Following initial stabilization, the patients were taken to the dressing room for reevaluation of the burned areas and debridement, escharotomy or fasciotomy, as indicated. The burn wounds were closed by using one of the local chemotherapeutic agents, such as silver sulphadiazine, mafenid acetate or silverincorporated amniotic membrane (SIAM) (6). In some of the cases, antacids and/or H2 receptor blocking agents were administered for the prevention of upper gastrointestinal (GI) bleeding. In cases of upper GI bleeding, a nasogastric catheter was inserted to irrigate the stomach, and antacids and/or H, receptor blocking agents and sedatives were given. Blood transfusions were administered as required. Surgical intervention became imminent in cases of failure of energetic conservative treatment. Results During the treatment of 915
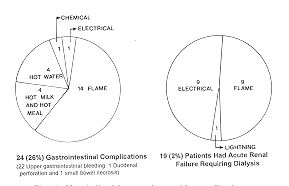
hospitalized patients, the following GI complications were encountered in 24 (2.6%)
patients: a 10-month-old female patient with hot water burn injury had duodenal
perforation; a 36-year-old male patient had massive small bowel necrosis due to electrical
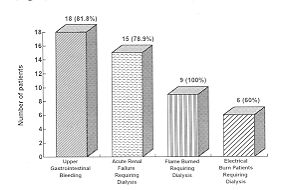
injury; and the other 22 patients had upper GI bleeding. The causes and average burn areas
in upper GI bleeding patients were as follows: 17 patients with flame burns (14 had an
average of 44.7% T13SA); 4 patients with hot milk and hot meal burns (with an average of
35.7% T`BSA), and one patient with chemical bums (74% TBSA). Eighteen of the 22 patients
with upper GI bleeding died (mortality rate 81.8%). Bleeding episodes lasted on average
10.1 days (range 1-14 days). Four of these deaths were due to massive bleeding, and the
others to septic complications. Sepsis was revealed in 7 patients on days 11 to 15. Four
patients were operated on in order to control the upper GI bleeding. Suturing of the ulcer
combined with vagotomy + pyloroplasty was performed in 3 patients, and vagotomy +
gastrojejunostomy in one patient.
The burn injuries in the patients
requiring dialysis varied statistically (p < 0.01). Of the 19 patients, one underwent
haemodialysis, 13 peritonea] dialysis, and 5 both haemodialysis and peritoneal dialysis.
In 14 patients, dialysis treatment was started on the first 3 days (mean 1.8), while the
other 3 patients underwent dialysis on days 7 to 13 post-burn (mean 9.6).
Death occurred on average on day 8 post-burn (range 2-20) as a result of sepsis. Death occurred 4.5 days on average after the onset of renal failure in ATN patients, and 2.5 days on average after the onset of MOE Discussion In burn patients, severe complication
such as sepsis, acute renal failure, GI bleeding, myocardial infarction, small bowel
necrosis, pulmonary embolus, duodenal perforation and adult respiratory distress syndrome
(ARDS), may be encountered (1,3,5,7,8). In our series the rate of acute renal failure
requiring dialysis was 2.6%, while gastrointestinal complications, such as upper GI
bleeding, duodenal perforation and massive necrosis of the small intestine, had a rate of
2.0%.
RESUME. Pendant une période de 11 années üanvier 1979-décembre 1989) 915 patients brûlés ont été hospitalisés chez notre centre. Comme liquide de réanimation nous avons employé la formule de Parkland pour tous les patients. Chez 24 (2,6%) patients nous avons observé des complications gastrointestinales (GI), dont 22 avec des complications de l'appareil GI supérieur. Nous avons effectué, chez 4 patients avec hémorragie massive d'un ulcère, la vagotomie + pyloroplastie ou la vagotomie + gastrojéjunostomie avec suturation de l'ulcère. Dix-huit des 22 patients avec hémorragie de l'appareil GI supérieur sont morts. Les causes du décès étaient l'hémorragie massive chez 4 patients et les complications septiques chez les autres. Dix-neuf (2%) des 915 patients brûlés ont nécessité la dialyse à cause d'insuffisance rénale aiguë. Les raisons de la nécrose tubulaire aigue étaient ou l'insuffisance organique multiple ou la sepsis. Le taux de mortalité chez les patients avec insuffisance rénal aiguë qui nécessitaient la dialyse était 78,9% (100% chez les patients brûlés par flammes et 60% chez les patients avec brûlures électriques), BIBLIOGRAPHY
|