| Ann. Medit. Burns Club - vol. VI - n. 2 - June 1993
SYNTHETIC SKIN SUBSTITUTE FOR SUPERFICIAL PAEDIATRIC BURNS Weiss J., Herman 0., Wertheym E., Shafir R. Department of Plastic Surgery Ichilov Hospital, Tel Aviv Medical Center, Sackler School of Medicine, Tel Aviv University, Israel SUMMARY. Most paediatric bums are small-sized and superficial. Conventional treatment consists of once or twice daily change of dressings, the application and removal of which is painful. To avoid the pain, emotional trauma and hospitalization (which is sometimes indicated to facilitate the treatment), new materials have been tried. Orniderm is a synthetic-polyurethane membrane. Its application and removal are easy and painless. The bum heals under this transparent sheet. There is no need for any further treatment, hospitalization is unnecessary and the child returns to its daily activities unrestricted. Most paediatric burns are small-sized burns of intermediate depth, requiring only local treatment. The changing of dressings and repeated visits to the hospital clinics for that purpose are a very traumatic experience for both the burned child and its parents (1, 2). The energy and costs of hospitalization, or ambulatory treatment, invested in dealing with these bums are high. It is therefore important to find ways of reducing these expenses. The local application of a dressing which does not have to be changed until complete healing of the bum should help in achieving that goal. Conventional treatment of second-degree burns Superficial and intermediate thickness seconddegree burns of up to 10-15% body surface area (BSA) can usually be treated on an ambulatory basis, depending. on the part of the body burned, the age of the child, the environmental conditions of its family and its general health. Not infrequently, the child is hospitalized for a short period until the depth of the burn is defined, which is at times difficult at the early stage, especially in scald burns (3). The bum has to be covered to avoid desiccation and secondary deepening. There are different modes of accepted treatment, such as:
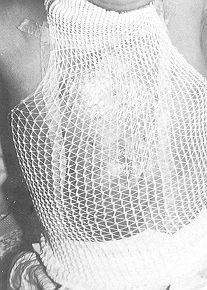
Physical characteristics of Omiderm Omiderm is a thin transparent polyurethane-based membrane. It is inelastic when dry, but highly flexible when wet. It has water permeability of about 5000g/ml/24 h. Omidertn sticks to the moist wound surface; however, since it does not have an adhesive material on its surface, it peels off easily when soaked. Application method After removal of the burned layers and cleansing of the wound, Orniderm is applied to the wound. The membrane can be used wet and flexible to cover uneven areas, or dry on smooth ones. If large quantities of fluid accumulate underneath the membrane, which may be the case in the first few hours post-injury, the membrane is replaced with pre-meshed sheet. The-. Omiderm sheets adhere well to each other. Small fluid collections are removed by stabbing the membrane. Once Omiderin sticks to the burn wound it is not changed, there is no pain, and the child is free to continue with its daily activities. It sometimes takes several hours for the membrane to adhere well to the wound surface. To avoid sheering of the sheets over the moist wound, these are held in place with adhesive tape (Figs. 1 and 2) or with a
Bandafix-elastic net (Figs. 3 and 4). Application should be limited to one circular sheet around a limb, to avoid a constricting effect when the membrane dries out on the bum. When the sheet is well adhered to the wound (Fig. 5), the child can be put under the shower. The Omiderm will come off only if soaked and actively peeled off. Once the bum has healed the membrane will come off with the underlying debris and burned tissue. Advantages of the synthetic skin substitute Orniderm The application and removal of Omiderm are painless. Its transparency facilitates easy observation of the bum wound, and reassessment of bum depth in poorly defined scald bums. It acting as a barrier between the wound and its
Wound healing is enhanced as is the case with other occlusive or semi-occlusive dressing materials (7,8). The cost of treatment of intermediate small area bums with the synthetic dressing is minimal, since no dressing change is needed, or hospitalization, or nursing. As soon as the bum has healed, the membrane peels off together with the debris. The greatest advantage of this dressing is the avoidance of painful, traumatic dressing changes and confrontations between the child and the medical team. Omiderm has also been used to cover fresh skin abrasions, skin donor-sites, lesions of congenital aplasia cutis (11) and as a temporary coverage of meningomyeloceles.
RESUME. La plupart des brûlures pédiatriques sont peu étendues et superficielles. Le traitement conventionnel consiste en le changement une ou deux fois par jour des pansements, ce qui est toujours douloureux pour l'enfant. Afin d'éviter la douleur, le trauma psychique et l'hospitalisation nous avons essayé un nouveau matériau. L'Omiderm est une membrane synthétique-polyuréthanne. L'application et l'enlèvement sont faciles et indolores. La brûlure se cicatrise au-dessous de la feuille transparente. Il n'y a plus besoin d'autre traitement, l'hospitalisation n'est pas nécessaire et l'enfant peut retourner sans gêne à ses activités quotidiennes. BIBLIOGRAPHY
|