| Ann. Medit. Burns Club - vol. 6 - n. 2 - June 1993
SHOULDER DISARTICULATION AFTER HIGH-TENSION ELECTRICAL BURNS: TECHNICAL PROBLEMS Belba G., Zhuka K, Osmani X., Gedeshi 1. Clinic of Plastic Surgery and Burns, U.C.H.T., Tirana, Albania SUMMARY. In our daily practice we have come across massive acute haemorrhage from the axillary artery or vein during the late postoperative period, in the proximity of the ligature, after shoulder disarticulation in high-tension electrical burns. In these cases the stabilization of haemorrhage is imperative. The ligation is performed at a distance from the subclavian artery and vein. In order to avoid both haemorrhage and a second operation (which in most cases is carried out as an emergency), during the same operation stage we first ligate the subelavian artery and vein with a subclavian separate incision, and then we perform shoulder disarticulation. Introduction The passage through the body of
high-tension electricity of 1000 V or greater causes irreversible injuries in the
extremities. The anatomical formations are very sensitive, being readily affected even at
a distance from the point of entry of the electric current. The technical evaluation of
major anatomical elements (muscles, vessels, nerves, etc.) is the main task of the medical
team. The definition of their destruction will determine the survival of the patient and
the complete or reduced function of the injured extremity. Materials and results An analysis of patients with high-tension electrical bums admitted during the period July 1990 - July 1992 to the Clinic of Plastic Surgery and Bums in Tirana shows a total of cases. The most typical localization was in the upper extremities, with 30 cases (Table 1). An examination of the distribution of amputation levels indicated that in 17 of these patients (56.6%) 18 amputations (Table 2) were performed. Shouder disarticulation was frequent, with 7 cases or 38.8% of the total number of amputations - this being a higher data than in other authors (1). LOCATION OF ELECTRICAL BURNS These seven patients had severe burns
of considerable extent varying from 10% to 25% BSA (mean 16.6%). In addition to shoulder
disarticulation other operations were performed in some patients (an average of 3. 1 %),
such as necrectomy, fasciotomy and skin grafts, in order to treat the various injuries.
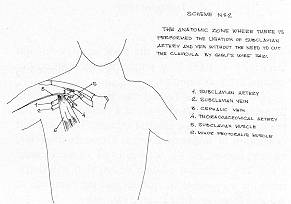
AMPUTATION AT THE UPPER EXTREMITIES we ligated the subclavian artery and vein, with a separate incision, and then performed shoulder disarticulation. The two patients confronted sepsis without any vascular complications (Fig. 2).
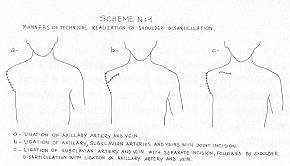
The hospitalization period of the patients subjected to shoulder disarticulation varied from 54 to 169 days, depending on the total injured surface, bum depth and the procedures applied. Of the seven cases, one patient died on the 20th day as a result of cerebral complications due to sepsis. Discussion In the septic conditions caused by electrotrauma there is a real danger of acute haemorrhage at the level where the extremity is amputated. This delayed haemorrhage usually takes place in the second week, when autolysis reaches its peak. Even if the amputation is performed on completely healthy tissue, because of tissue renecrotization the many secreions and the microthrombi dissolving in the area can cause the release of the ligation of the arterial or venous stump. If we divide the seven cases described above into sub-groups, this will allow us to discuss the technical intervention of shoulder disarticulation in order to eliminate acute delayed haernorrhage. Shoulder disarticulation with ligation of only the axillary artery and vein never excluded the danger of haemorrhage in these critical patients (Scheme l/a, Fig. 1). Ligation at a distance from the subclavian artery and vein during the same operation stage, but with joint incision together with disarticulation, created a relatively safer condition (Scheme I/b, Fig. 1). This is due to the fact that a secondary infection in the disarticulation zone per continuitatem will influence the ligation of the subclavian artery and vein, because the incisions and anatomical planes where the operation is performed are adjacent. We are of the opinion that the performance, from the beginning, of ligation of the subclavian artery and vein with a separate subclavian incision followed by shoulder disarticulation, with ligation of the axillary artery and vein, creates a safe post-operative situation (Scheme I/c, Fig. 1). Any infection would not be life-threatening and would be well tolerated because the incisions and subclavian anatomical plans and those of disarticulation have no connection points. In the four cases in which we performed ligation of the subclavian artery and vein, either as a secondary intervention in emergency or as a primary intervention during the same operation stage, we noticed a stability of the local condition and a normal course of the patient without any danger o haemorrhage. The operation technique of shoulder disarticulation with ligation at the beginning of the subclavian artery and vein has many general and specific aspects, from the incision lines which frequently are atypical to the angiological ligation of the vessels (7). We would underline the isolation moment of the subclavian artery and vein. The subclavicular incision involves the lateral third of the clavicle. The major pectoralis muscle is dissected, opening a window between the minor pectoralis muscle and the subclavian muscle. Thorough dissection will reveal at the beginning the subclavian vein and under this the subclavian artery. The ligation can be performed under the subclavian muscle at the level of the external side of the first rib, over the entry point of the cephalic vein and over the exit point of the thoracoacromial artery (Fig. 2). Cutting of the clavicle by Gigh's wire saw is not necessary. Lastly we would recommend that during shoulder dis articulation, the deltoid muscle should be protected as much as possible, because if it is uninjured it can ensure closing per primam of the wound. RESUME. Nous avons observé dans la pratique de tous les jours des cas d'hémorragie massive aiguë de l'artère ou la veine axillaire après la désarticulation de l'épaule, à la suite des brûlures électriques. Chez ces patients la stabilisation de l'hémorragie est assolument nécessaire La ligature est effectuée à distance de l'artère et la veine sous-clavière. Pour éviter soit l'hémorragie soit une seconde intervention (effectuée généralement en urgence), pendant la même opération, après avoir lié l'artère et la veine sous-clavière avec une incision sous clavière séparée, nous effectuons la désarticulation de l'épaule. BIBLIOGRAPHY
|