| Ann. Medit. Burns Club - vol. 6 - n. 2 - June 1993
REHABILITATION OF ELDERLY BURNED PATIENTS: POSSIBILITIES AND LIMITS Amico M., Geraci V., Mingoia S., Masellis M. Divisione di Chirurgia Plastica e Terapia delle Ustioni, Ospedale Civico USL 58, Palermo, Italy SUMMARY. The rehabilitation of the elderly burned patient presents a series of problems, which are considered in this paper. These problems are both physical and psychological and any rehabilitation programme must take them into account. The Palermo Bums Centre has a two-phase protocol, for the hospitalization period and for the long post-discharge period. The first of these prescribes appropriate posture training, early mobilization and intensive occupational therapy. In the second phase, on discharge, patients are assigned to one of three distinct groups according to their age and condition. The ultimate objective is the maintenance of muscular strength, the prevention of articular stiffness and postural vices, and the strengthening of motor function. The various phases are described, always bearing in mind the particular physical and psychological limitations of the elderly. Introduction From the point of view of prognosis
and functional recovery, the bum trauma is probably the most serious injury that can
affect elderly persons. In such patients, even if the burns are not extensive, the
treatment for psychophysical rehabilitation is of fundamental importance in order to
guarantee a good quality of residual life. The programme of recovery is complicated by a
series of physiological and psychological factors (1). Factors limiting rehabilitation of the elderly The physicalfactors (2, 3, 4) that exert a negative
influence on recovery are: paramorphism of the lower limbs, senile kyphosis, limitation of
articular excursion and motor activity, chest deformation and neuromotor deficit. Rehabilitation programme The preparation of a valid "personalized"
programme of rehabilitation treatment has to be preceded by a careful anamnesis in order
to assess previous motor limitations, the presence of degenerative diseases, pre-existing
deformities, pain phenomena, intellectual level and psychological disturbances, together
with the family and economic background and the patient's previous social relations
(1,2,5,7).
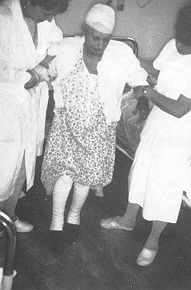
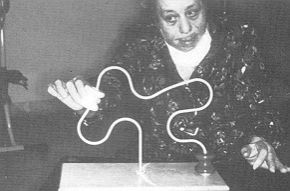
do not fatigue the patient, provoke as little pain as possible, and perform only short but frequent sessions. It is important to inform patients of the purposes of the therapy, which they tend to refuse because of the pain it causes. Mobilization will help to reduce pressure sores and articular problems. The prevention of ulcers is guaranteed by continuous posture change, by water- and air-beds and by hammocks which with their rotating sides help to change the patients' position easily and ainlessly (Figs 1, 2). The patients are encouraged to get up from their beds as soon as possible, with the aid of elastic bandaging of the limbs. This helps to maintain capillary tone, to reduce osteoporosis due to immobilization, to facilitate renal function, to improve puh-nonary ventilation, to maintain muscular tone and above all to restore the patients' confidence in themselves and their recovery (Figs. 3, 4). The prevention of articular problems (3, 4, 5, 6) is effected by means of exercises of physiokinesis therapy in all its aspects: passive, active, active assisted and resistance, both in bed and in the swimming-pool or gymnasium. Hydrotherapy produces particular beneficial effects and is well tolerated because the patients are immersed in water and can perform their exercises with less physical effort and are therefore more willing to co-operate. In the final period of hospitalization, rehabilitation coming and different from that of intensive care where the patient has long been kept in isolation, and it will allow him to re-establish contact with the outside world and prepare him sychologically for his discharge and his return to the family, Elderly patients are often unwilling to return home either because they are afraid they will not receive adequate care and support from their family or because they begin to look upon themselves as being permanently ill and requiring special care. They therefore believe that the hospital environment is where they will best be protected.
Recreational pastimes such as basketwork,
carpet making, drawing and painting, together with card therapy is performed in the
gymnasium. This games, bingo, etc., all serve to stimulate the environment is new to the
patient: it is wel attention and above all to help socialization. Conclusion The particular psychological and
physical conditions of the elderly person who has suffered burn injuries and has to go
through functional recovery treatment play an important part in the preparation of the
rehabilitation programme and in its realization. RESUME. La réadaptation des patients brûlés âgés présente une série de problèmes que les auteurs considèrent. Ces problèmes sont de nature physique et psychologique et tout programme de réadaptation doit en tenir compte. Le Centre des Brûlés de Palerme a un protocole à deux phases, pour la période de l'hospitalisation et pour la longue période de la convalescence. La première phase prescrit des exercises appropriés pour la posture, une mobilisation précoce et une thérapeutique occupationnelle intensive. Dans la deuxième phase, après le renvoi de l'hôpital, les patients sont divisés en 3 groupes, selon l'âge et la condition physique. Le but final est le maintien des forces musculaires, la prévention de la rigidité articulaire et les vices de posture, et le renforcement de la fonction motrice. Les auteurs décrivent les différentes phases, en tenant toujours compte des particulières limitations physiques et psychologiques du patient âgé. BIBLIOGRAPHY
|